Ovary
Introduction
What is cancer?
Cancer is a disease of the body’s cells. Our bodies are constantly making new cells to grow, to replace worn-out ones, or to heal damaged ones after an injury. Normally, cells grow and multiply in an orderly way. Occasionally, however, some cells behave abnormally. They multiply in an uncontrolled way, and these abnormal cells may grow into a lump which is called a tumour.
http://healthgate.partners.org/images/exh4463.jpg
Tumours can be benign (not a cancer) or malignant (a cancer). Benign tumours do not spread outside their normal boundary to other parts of the body. A malignant tumour is made up of cancer cells. If these cells are not treated they may spread into surrounding tissues.
If the abnormal cells invade (spread) beyond their normal boundaries then the tumour is malignant, that is, it is a cancer.
Sometimes cells break away from the original (primary) cancer and spread to other organs. When these cells reach a new site in the body, they may continue to grow and form a new tumour on that site. This is called secondary cancer or metastasis
Tumours can be benign (not cancerous) or malignant (cancerous). Benign tumours do not spread outside their normal boundary to other parts of the body. A malignant tumour is made up of cancer cells. If these cells are not treated they may spread into surrounding tissues.
If the tumour cells spread beyond their normal boundaries then the tumour is malignant, that is, it is a cancer.
Sometimes cells break away from the original (primary) cancer and spread to other organs. When these cells reach a new site they may continue to grow and form another tumour at the site. This is called a secondary cancer or metastasis.
In some cancers, it is the body's blood cells, which multiply abnormally. These cancers are called leukaemia myeloma and lymphoma.
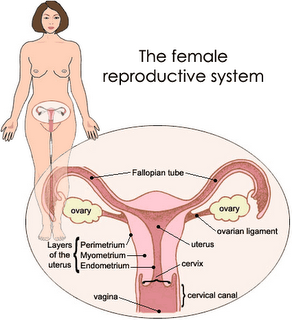
The ovaries
The ovaries are part of the female reproductive system and contain eggs (ova) which can make a new human life when fertilised. In women of childbearing age, a mature egg is released from one of the ovaries each month (ovulation) and travels down the Fallopian tubes to the uterus (womb)
The ovaries are almond shaped organs, each about 3 cm long and I cm thick. They are found inside the pelvic cavity, one on each side of the uterus and are very close to the end of the Fallopian tubes.
Each ovary has an outer covering made up of a layer of cells called epithelium. Inside are 'germ cells' which will eventually mature into eggs. The eggs travel to the outside of the ovary to be released into the Fallopian tubes. If the egg is not fertilised by male sperm, it passes out of the uterus with the monthly period (menstruation).
The ovaries also contain cells which release the female hormones: oestrogen and progesterone. These cells are called 'sex cord stromal' cells.
As women get older, the ovaries gradually produce less oestrogen and progesterone. At the same time the production of eggs also decreases and the woman's periods become irregular and eventually stop. This is known as menopause, or the 'change of life', and usually happens between the ages of 45 and 55. After menopause it is no longer possible to have a child.
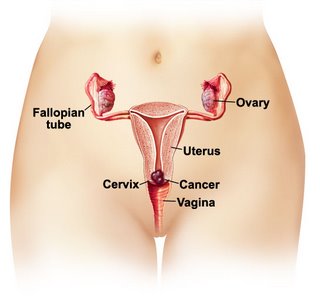
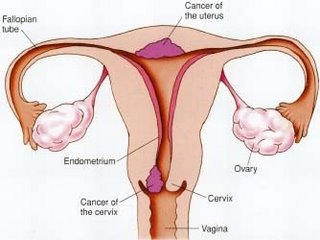
Ovarian cancer
Ovarian Cancer is a malignant tumour in one or both ovaries. There are four main types of ovarian cancer, named after the part of the ovary that is affected. Knowing exactly which type of cancer you have helps your doctor advise you on which treatment is best for you.
Epithelial ovarian cancer
This type of ovarian cancer arises in the epithelium: the outer cells covering the ovary. It is the most common type of ovarian cancer. Nine out of 10 ovarian cancers are epithelial.
Germ cell and sex cord stromal cell ovarian cancers
These two types of ovarian cancer are very uncommon. The germ cell cancers arise in the cells that mature into eggs and usually only affect women under 30 years of age.
Sex cord stromal cell cancers arise in the cells which release the female hormones. These cancers can occur at any age.
Germ cell and sex cord stromal cell ovarian cancers usually respond very well to treatment and are often curable. If these cancers only affect one ovary, it may still be possible for younger women to have children after treatment.
Borderline tumours
Borderline tumours are a group of epithelial tumours which are not as aggressive as other forms of ovarian cancer. Sometimes the words 'low malignant potential' are used to describe borderline tumours
The outlook for women with borderline tumours is generally good regardless of whether the disease is diagnosed early or late.
Cancer of the Fallopian tubes
Rarely, cancer develops in the Fallopian tubes. This is very similar to epithelial ovarian cancer and is treated in much the same way.
How common is ovarian cancer?
About nine out of 10 ovarian cancers occur in women over the age of 40 years. Like most cancers, the risk of ovarian cancer increases with age.
Causes of ovarian cancer
The causes of most ovarian cancers are not known. Some factors seem to put women at a higher risk of developing ovarian cancer. Many women who develop ovarian cancer do not have these risk factors. At the same time many women who do have the risk factors do not develop ovarian cancer.
Ovarian cancer is more common in Caucasian (white) women who live in Western countries with a high standard of living.
Women who have no or few pregnancies appear to be more at risk of ovarian cancer. Women who have taken the contraceptive pill for a number of years seem to be at less risk. The exact reason is uncertain. It could be that ovarian cancer is more likely to develop when the ovaries do not have a 'rest' from ovulation (release of eggs) during a woman's lifetime.
Women who have no of few pregnancies appear to be more at risk of ovarian cancer. Women who have taken the contraceptive pill for a number of years seem to be at less risk. The exact reason is uncertain. It could be that ovarian cancer is more likely to develop when the ovaries do not have a 'rest' from ovulation (release of eggs) during a woman's lifetime.
Some types of ovarian cancer may be linked with a family history of cancers of the ovary, bowel, breast and lining of the uterus. Between five and 10 per cent of ovarian cancers are caused by inheriting a damaged gene from a parent. If you are concerned about this, talk with your doctor.
Other risk factors for ovarian cancer, which have been suggested include a high fat diet, using talcum powder around the genital area and the mumps virus. The link between these factors and ovarian cancer has not been proved.
Diagnosis
The early symptoms of ovarian cancer are vague. They can be caused by other problems, so it is very difficult for you or your doctor to suspect they are due to ovarian cancer. Sometimes ovarian cancer is found unexpectedly during an operation such as a hysterectomy
Symptoms
Symptoms of ovarian cancer can include a feeling of discomfort in the abdomen or a bloated feeling or pressure. There may be a change in bowel habits and flatulence (wind). Indigestion is also common and sometimes problems with the kidneys or bladder. Some women have abnormal vaginal bleeding. Occasionally pain may be the first sign of ovarian cancer.
As the tumour grows, your abdomen can become quite enlarged. This is caused by the tumour itself or sometimes by a build up of fluid called ascites. Ascites develops in response to the tumour in the abdomen. Loss of weight may also occur in spite of having an enlarged abdomen.
There is currently no effective way to detect ovarian cancer early. Unfortunately the Pap test is only effective for the early detection of cancer of the cervix. Much research is being carried out to look at new ways to find ovarian cancer early.
Many women feel angry or upset that their illness was not discovered earlier. You may even feel guilty that you did not go to a doctor sooner. It is quite normal to have these feelings and it may help you to talk about them with your doctor or nurse.
What doctors and other health professionals will I see?
Your general practitioner will refer you for initial tests to confirm whether or not you have cancer. He or she may later refer you to a specialist who will advise you about treatment options.
Specialists and other health professionals who care for people with ovarian cancer include:
gynaecological oncologists: diagnose and treat people with ovarian cancer
medical oncologists: responsible for chemotherapy
radiation oncologists: responsible for radiotherapy
surgeons: responsible for some biopsies and other surgical procedures
dieticians: recommend the best diets to follow while you are in treatment and recovery
nurses: assist you through all stages of your hospitalisation and cancer experience
social workers, physiotherapists and occupational therapists: advise you on support services and help you to resume normal activities.
How ovarian cancer is diagnosed
If ovarian cancer is suspected or has been diagnosed, you will need to be referred to a gynaecologist who specialises in treating women with ovarian cancer, a gynaecological oncologist. Your specialist will arrange for you to have a number of tests and examinations. These tests help the doctor decide whether your symptoms are due to ovarian cancer or to other causes.
Physical examination
This will include an internal pelvic examination where the doctor checks for a mass or lump in the lower abdomen.
Blood tests
Blood can be tested for a particular protein or a tumour marker called CA 125. This protein is often higher than normal in women with ovarian cancer. Some women may have other tumour markers called 'inhibin' or 'CEA'. The type of marker depends on the type of tumour. However, some tumours will not have any of these tumour markers.
Testing your blood for these tumour markers is one way to help diagnose cancer. These tests are also used later on to check the progress of your illness.
Other blood tests may be taken to help with your diagnosis and to check the effects of treatment.
X-ray and other imaging tests
Routine chest and abdominal x-rays may be taken.
Ultrasound scans are very important in the diagnosis of ovarian cancer. These are done in two ways. You may have an abdominal scan, where the ultrasound specialist passes a handheld device called a transducer over your pelvic area. This is used to build up pictures of your organs, which can be seen on a screen. You may also have a trans-vaginal ultrasound, where the transducer is inserted into your vagina. This is because the ovaries sometimes cannot be imaged by the abdominal ultrasound. Some women find the procedure a little embarrassing and uncomfortable, although it is not painful. Discuss the procedure with your doctor and ultrasound specialist if you have any concerns.
You may also have an x-ray of your bowel to make sure that your symptoms are not due to a bowel problem. This x-ray is called a barium enema, which is not painful but can be rather uncomfortable. With a barium enema, special fluid is inserted into your bowel through your back passage (rectum) and x-rays are then taken.
Unfortunately, none of these tests can definitely diagnose ovarian cancer. The only way this can be done is with an operation. This means that ovarian cancer is usually diagnosed and treated at the same time.
You need to make sure that you understand enough about your illness and the operation before you have your surgery.
The stages of ovarian cancer
Like all cancers, ovarian cancer can spread to other parts of the body. However, ovarian cancer tends to spread within the abdominal and pelvic cavities rather than to more distant parts of the body. As the tumour grows larger, tumour nodules or seeds can invade other organs near the ovaries. These include the bowel, appendix, bladder, omentum (a protective membrane of fatty tissue which covers the abdominal organs), diaphragm, lymph nodes and liver.
If the ovarian cancer you have is confined to the ovaries or very close to the ovaries, it may be called stage I or II. If it has spread to other organs it may be stage III or IV. Knowing the stage of the disease helps your doctor discuss treatment choices with you.
Treatment
Treatment for ovarian cancer usually involves surgery and chemotherapy. It may also include radiotherapy.
Surgery
The first treatment for ovarian cancer is usually an operation called a laparotomy. In this operation a long vertical cut is made in your abdomen which allows your doctor to find and remove as much tumour as possible.
In many cases, your doctor will do a biopsy of the tumour at the beginning of the operation to make sure it is a cancer. This is called a 'frozen section’. If cancer is confirmed, the operation will continue. For most women the operation will then involve the removal of the ovaries and Fallopian tubes, the uterus, the omentum (the 'apron' of fatty, protective tissue covering the abdominal organs), the appendix and some of the lymph nodes in the area. Sometimes it is necessary to remove part of the bowel.
After the operation, samples of tissue from the ovary itself, pelvic lymph nodes and other organs are sent to a laboratory for further examination. The results of these biopsies will provide more information about the type and extent of your cancer. This information is necessary before you and your doctor can make decisions about further treatment after the operation.
It may sound as if a lot of your body parts or organs are removed in the operation. However, these organs are quite small compared with everything else in your abdomen and pelvis and their removal will not leave a space.
For some women, the operation and the scarring may not be so extensive. For instance, a young woman with an early ovarian cancer or borderline tumour may not need to have her uterus and both ovaries removed. In this case it may still be possible for her to have children.
After the operation
When you wake up from the operation, you will find that you have several tubes in place. You will have an intravenous drip, which will give you fluid as well as medication. One or two tubes may have been inserted into your abdomen to drain away any fluid from the operation site. You will also have a catheter in your bladder to drain away urine. As you recover after the operation, these tubes will be removed, usually within three to five days.
As with all major operations, you will experience some discomfort or pain. You will have pain relievers to control this. They may be given through an intravenous drip or through an epidural tube into your spine. This epidural pain relief is similar to that given to women during childbirth. It is best to let your nurse know when you are starting to feel uncomfortable: don't wait until the pain becomes severe.
This operation is a major one and you may be in hospital for about one week. Before you go home, your doctor will have the results of your biopsies and will discuss further treatment with you. This will depend on the type of cancer, the extent of disease and the amount of any remaining cancer. Further treatment, usually chemotherapy, is almost always needed for ovarian cancer.
Chemotherapy
Chemotherapy is the treatment of cancer using anti-cancer drugs. The aim is to destroy cancer cells while causing the least possible damage to normal cells. The drugs kill cancer cells by stopping them from multiplying.
Chemotherapy works best when the tumour is small and the cancer cells are actively growing. With ovarian cancer, even though most of the cancer may have been removed at the time of the operation, there may be some cancer cells left. For this reason, chemotherapy works best if it is started soon after the operation.
Chemotherapy is usually given through an intravenous drip. Your first treatment may be given while you are still in hospital, or a few days later. You will have one treatment every three to four weeks for a total of six sessions, or a variation of this. You may be required to stay in hospital overnight, but it is more likely that you will be treated as a day patient. This depends on the drugs you are given and how you are feeling. Blood tests are taken before each treatment to ensure your body's normal cells have had time to recover.
During your chemotherapy you may have other blood tests to monitor the effectiveness of the treatment. The doctor may look for the CA 125 tumour marker, which involves a simple blood test. After your third course of chemotherapy you may also have a CT scan to check that you are responding to treatment. The CT scan is usually done at a hospital or a special clinic. You do not need to be admitted to hospital and you should have no side effects. The scan involves taking x-rays at different positions so that a two and three-dimensional image of the body can be built up.
Before the scan you will be asked to drink some fluid that shows up on x-rays. This makes it easier for abnormalities to be detected. Your doctor will discuss the results of these tests with you.
If your ovarian cancer does not respond completely to a particular type of chemotherapy, or if your disease comes back, other drugs are available. These include drugs such as Taxol.
Side effects of chemotherapy
The side effects of chemotherapy differ according to the particular drugs used. They may include feeling sick or off-colour and tired and some temporary thinning or loss of hair. Your hair will grow back when treatment is completed.
You may also find yourself more at risk of infections. These side effects are usually temporary and measures are always taken to either prevent or reduce them.
If you are treated with Taxol you may find that you have joint and muscle pain, rather like flu symptoms, for a few days after treatment. These symptoms usually disappear after a few days. You may also find that you get numbness or tingling in your hands and feet. Let your doctor know if this happens to you.
Radiotherapy
Radiotherapy (treatment using radiation) is occasionally used for women with ovarian cancer, especially if it is confined to the pelvic cavity. If radiotherapy is advised, your doctor will discuss it with you.
Further surgery
After your last chemotherapy treatment, you will have more blood tests and a CT scan. You will also have a physical examination. If your treatment has had a good effect and there is no obvious sign of cancer your doctor may discuss the need to have another operation. In this operation more biopsies are taken just to be sure. This is called a 'second look operation'. It may be a small one known as a laparoscopy or a bigger operation similar to your first one.
You will need to discuss the advantages and disadvantages of this second operation with your doctor.
Further chemotherapy
Further chemotherapy may be needed if your cancer does not respond completely to your initial treatment. It may also be needed if your disease comes back sometime in the future. The drugs that may be used will depend on what drugs you have previously had, as well as the aims of the treatment.
Palliative care
If the cancer has spread and it is not possible to cure it, then your doctor will discuss various treatments for specific problems caused by the cancer.
Palliative treatment is treatment that relieves or soothes pain and other symptoms of illness. Palliative care is available for all people who experience pain and distress associated with cancer, whatever their stage of cancer treatment. It is a particularly important type of treatment for people with advanced cancer, who cannot be cured but can expect to live without undue pain and distress.
Palliative care includes pain relief using painkilling drugs and other measures. Pain is usually well controlled with oral medication. If pain is particularly severe or difficult to control, then you may have injections of pain-relieving medication.
General practitioners, specialists and specialist palliative care teams in hospital all play important roles in palliative treatment for people with early and advanced cancer. For further information, contact the Resource & Wellness Centre at 03 – 2698 7300 or email contact@cancer.org.my.
Prognosis/outlook
The outlook (or 'prognosis') for women with the less common types of ovarian cancer (for example, borderline tumours or germ cell tumours), is usually very good. For women with the more common epithelial ovarian cancer, it is not so easy to predict the outcome.
Like most cancers, ovarian cancer can often be cured. Many women, even with advanced disease, respond very well to treatment, however repeated chemotherapy treatments and surgery may be necessary to achieve this.
A diagnosis of cancer can make your future seem very uncertain: it may help to think of it as a chronic illness. This means that even if your cancer cannot be cured it can still be treated. You can then return to a near normal life for long periods of time.
If you would like information about your own outlook, you need to speak to your specialist who is familiar with your medical history.
If any relapse or repeat of your symptoms occurs, you should always consult your specialist, as you may need more treatment.
Making decisions about treatment
Sometimes making decisions about the right treatment for you can be very hard. You may feel that everything is happening too fast, that you don't have time to carefully think things through.
While some women feel they are overwhelmed with information, others may feel that they don't have enough. You need to make sure that you understand enough about your illness, the possible treatment and side effects to make your own decisions.
For some women with ovarian cancer, treatment will result in a cure. However, treatment often means that women can no longer have children. This may be a blow for many women even if they already have a family. For other women who have not yet had children, it can be devastating. When fertility is really important for you, talk with your doctor about what other choices may be available to you. This will depend on the type of ovarian cancer you have.
For other women with more advanced ovarian cancer, treatment may be aimed at controlling symptoms rather than curing the cancer. Sometimes, the best way to control the symptoms is to treat the cancer, which may carry a small chance of a cure. Some women in this situation want all possible treatments, while others want to make sure that the possible benefits of treatment will outweigh the possible side effects. Still others will choose the option they consider offer them the best quality of life.
Talking with doctors
If it is suspected that you have ovarian cancer, you may find that things move very rapidly. This makes it very hard for you to make your decisions. It is also very difficult to take everything in, and you may need to ask the same questions more than once. You may find it helpful to talk not only with your doctor(s), but also with the nursing staff who will be caring for you during your initial treatment. You have the right to find out what a suggested treatment means for you and the right to accept or refuse it.
Talking with others
Once you have discussed your treatment options with your doctor, you may want to talk them over with your partner, family or friends, the nursing staff, the hospital social worker, or your own spiritual or religious adviser.
Talking it over can help to sort out what course of action is right for you.
You may be interested in looking for information about ovarian cancer on the Internet. The Internet offers a massive amount of useful information. However searching for information on an. issue as personal as your health can produce thousands of websites with no assurance that the information is credible or reliable. We recommend that you begin with the National Cancer Society of Malaysia’s site (www.cancer,org.my) and use our links to find other good cancer websites.
The Resource & Wellness Centre also has trained staff available to talk to people who phone or walk in, and they can refer you to other sources of information and help. Telephone 03 – 2698 7300.
A second opinion
You may also want to ask for a second opinion from another gynaecological-oncologist. This is understandable and is your choice. Your specialist or local doctor can refer you to another specialist for this. You can still ask for a second opinion even if you have already started treatment and still want to be treated by your first doctor.
Taking part in a clinical trial
Your doctor may suggest that you consider taking part in a clinical trial.
Clinical trials are a vital part of the search to find better treatments for cancer. Doctors conduct clinical trials to test new or modified treatments and see if they are better than existing treatments. Many people all over the world have taken part in clinical trials that have resulted in improvements to cancer treatment. For ovarian cancer patients these trials have resulted in treatments, which significantly improve women's amount and quality of life. However the decision to take part in a clinical trial is always yours.
If your doctor asks you to take part in a clinical trial, make sure that you fully understand the reasons for the trial and what it means for you. Before deciding whether or not to join the trial, you may wish to ask your doctor:
What treatments are being tested and why?
What tests are involved?
What are the possible risks or side effects?
How long would the trial last?
Will I need to go into hospital for treatment?
What will I do if any problems occur while I am in the trial?
If you decide to join a randomised clinical trial, you will be given either the best existing treatment or a promising new treatment. You will be chosen at random to receive one treatment or the other, but it will always be at least the best treatment available,
If you do join a clinical trial, you have the right to withdraw at any time. Doing so will not jeopardise your treatment for cancer.
It is always your decision to take part in a clinical trial. If you do not want to take part, your doctor will discuss the best current treatment choices with you.
Recovery and follow-up care
Recovering from treatment is different for each woman. It depends on the type and stage of ovarian cancer you have and also the amount of treatment you have needed.
You will need to have regular check-ups with your specialist. These may include blood tests, x-rays and ultrasound, and physical examinations. Talk with your doctor about how often these may be.
It may take some time for you to recover from the various types of treatment. You will find that there are physical changes as well as many emotional changes to cope with. It is important that you, your partner and family are prepared for this. You may also need to talk with your employer about how the treatment may affect your work.
Coping with side effects
It may take some time to recover from the various types of treatment. You will find that there are physical changes as well as many emotional changes to cope with. It is important that you, your partner, family and employer are prepared for this.
Tiredness
Many women complain that tiredness is a major problem. This is hardly surprising, as most women need chemotherapy before they have had time to recover from their operation. Travelling backwards and forwards to hospitals and clinics for treatment is also very tiring. If you start work again during the treatment and/or you have a home and family to care for, you will almost certainly find that you are very tired. If you are on your own and have to do everything yourself, tiredness will also be a problem.
Your tiredness may continue for quite a while even after treatment has finished. Some women find that it takes them up to one or two years to feel really well again. It may help to talk with your family and friends about how you feel and discuss ways in which they can help you. You may need to plan your activities during the day so that you get regular periods of rest.
Premature menopause
If you have had both your ovaries and your uterus removed, you will no longer have your periods and it will not be possible to become pregnant. If you have not been through menopause already, you may experience premature menopause. Because your ovaries have been removed suddenly, menopausal symptoms such as hot flushes and vaginal dryness could be more sudden than they would be with a natural menopause. You will need to talk with your doctor about the need for hormone replacement therapy.
Hormone replacement therapy may be given to control the symptoms of menopause. Oestrogen, a female hormone normally produced by the ovaries, is given to replace your natural oestrogen. Hormone replacement therapy can 'also reduce the risk of heart disease and osteoporosis (thinning of the bones) in the future.
Some women, however, are concerned that hormone replacement therapy may increase their risk of cancer, in particular breast cancer. The evidence about this is unclear. While many studies do not show any increased cancer risk after several years of hormone replacement therapy, there are still some unanswered questions.
You will need to discuss the issues with your doctor and weigh up the benefits and possible risks for yourself. There are also many useful books about menopause, which may help you with your decisions.
Bowel problems
It is not uncommon to have bowel problems after surgery for ovarian cancer. These can occur for some time after treatment. This may include diarrhoea, cramps or constipation. In particular, it is important not to become constipated. Talk with your doctor, nurse or the dietician about ways you can prevent constipation, and relieve any other symptoms.
Sometimes the bowel becomes blocked because of the surgery you have had. It may also occur because the cancer has come back. This blockage is called a bowel obstruction. If you have symptoms such as feeling sick, vomiting, abdominal discomfort or pain you should see your doctor or specialist as soon as possible. Quite often a bowel obstruction can be relieved with simple treatment in hospital. Occasionally you may need another operation to relieve your symptoms.
Lymphoedema
Lymphoedema is swelling of a part of the body, usually the arms or legs. It may occur after treatment for ovarian cancer if you have had some of the lymph nodes in your pelvis removed (a lymphadenectomy). Removal of the nodes may prevent normal draining of the fluid from the legs. As a result fluid can build up in one or both legs, causing swelling. This usually does not occur until some time after the operation.
It is not possible to predict whether you will have problems with lymphoedema. You should seek advice from your specialist or nurse and you may be given special stockings to wear after your operation.
Some hospitals have a specialist physiotherapist or nurse who can advise you on how you may be able to reduce your risk of developing lymphoedema. They can also help you manage if lymphoedema does occur in the future.
Ascites
Ascites is a collection of fluid in the abdominal cavity. This can be uncomfortable because of swelling and pressure. If it becomes a problem there is a simple procedure to drain away the fluid and relieve discomfort. This is called a 'paracentesis'. It is usually done on the hospital ward and you may need to stay overnight.
Pleural effusion
Sometimes fluid can also collect in the lining of the lungs. You may feel short of breath and have some pain. Again this fluid can be drained away to give you relief.
Seeking Support
It is normal to feel a range of intense emotions for some time after your diagnosis and treatment. You may feel sad, depressed, angry or frustrated. It is important to acknowledge these reactions and understand that it may take some time before you feel well again. It may be helpful to talk about your feelings with your partner, family members or friends or with a hospital counsellor, social worker, psychologist or your religious or spiritual adviser.
Sometimes you may find that your friends and family do not know what to say to you: they may have difficulty with their feelings as well. Some people may feel so uncomfortable that they avoid you. They may expect you to 'lead the way' and tell them what you need. This can be very difficult to bear and can make you feel very lonely. You may feel able to approach your friends directly and tell them what you need. You may prefer to ask a close family member or a friend to talk with other people for you.
Loss of fertility can be difficult for many women to cope with, even if they already have a child or children, or have chosen not to have children. You, with or without your partner, may need to seek help to cope with your grief. This may be through a social worker, psychologist or psychiatrist or through other support services.
Permanent care or adoption of a child may be a choice for some women. This requires dedication and perseverance and not all couples who wish to adopt a child are able to do so.
Diet
A balanced, nutritious diet will help you keep as well as possible and cope with the cancer and any side effects of treatment. Depending on the kind of treatment you have had, you may have special dietary needs. A dietician can help plan the best foods for your particular situation - ones that you find tempting, easy to eat and nutritious.
Exercise
You will probably find it helpful to stay active and to exercise regularly if you can. The amount and type of exercise you do will depend upon what you are used to and how well you feel.
Discuss with your doctor what is likely to be best for you.
Relaxation techniques
Some people find relaxation or meditation helps them to feel better. The hospital social worker or nurse will know whether the hospital runs any programs, or may be able to advise you on local community programs. The Resource & Wellness Centre also runs “Wellness Programmes” for those with cancer and their carers. Call 03 – 2698 7300 or email contact@cancer.org.my for more information.
Sexuality and cancer
The diagnosis and treatment of ovarian cancer may affect how you feel about yourself and your relationships. It is a time when you will need support as your relationships may change. Current or new partners may also have difficulty adjusting and may need reassurance.
If you are able to share your feelings with each other, you will find this helpful. However, this is not always possible. As with all crises, some relationships suffer under the strain. You may both need to seek separate support for yourselves.
If you are without a partner you may be concerned about forming new relationships. Talking about this with a close friend or an outside person such as social worker may be helpful.
Same sex partners may find they have an increased sense of vulnerability about their own bodies and health, when faced with the impact and uncertainty of their partner's illness.
Sharing affection with your partner through kissing, caressing and touching can give you both much pleasure. Talking about your needs together is important to help you feel more confident and to reduce any fears.
If you have any concerns about regaining your usual pattern of sexual activity, talk with your doctor or nurse. For some people, specialist help may be needed. For others, just a little practical, simple advice is needed, such as using KY Jelly for vaginal dryness.
Cancer support groups
Cancer support groups offer mutual support and information to people with cancer and, often, to their families. It can help to talk with others who have gone through the same experience. Support groups can also offer many practical suggestions and ways of coping.
Caring for someone with cancer
Caring for someone with cancer can be very stressful, particularly when it is someone you care about very much. Look after yourself during this time. Give yourself some time out, and share your worries and concerns with someone outside.
You may have to make many decisions. You will probably have to attend many appointments with doctors, support services and hospitals. Many people have found it helpful to take someone with them. It also helps to write down questions beforehand, and to take notes during the appointment.
Cancer support group membership is generally open to patients and carers. A support group can offer the chance to share experiences and ways of coping.
Resource & Wellness Centre
The Resource & Wellness centre is a service of the National Cancer Society of Malaysia. It is an information and support service for people affected by cancer. It is a confidential service where you can talk about your concerns and needs with specially trained staff. The staff can provide you with written information and can put you in touch with appropriate services in your own area. Telephone
03 – 2698 7300 or email contact@cancer.org.my for more information.
Information Checklist
You may find the following checklist helpful when thinking about the questions you may want to ask your doctor about illness and treatment.
What type of cancer do I have?
How extensive is my cancer?
What treatment do you advise for my cancer and why?
Will a doctor who specialises in ovarian cancer perform my treatment (and surgery)?
Are there other treatment choices for me? If not, why not?
What are the risks and possible side effects of each treatment?
Will I have to stay in hospital, or will I be treated as an outpatient?
How long will the treatment take? How much will it affect what I can do?
How much will it cost?
Will I have a lot of pain with the operation? What will be done about this?
If I need further treatment, what will it be like and when will it begin?
Will the treatment affect my sexual relationships?
How frequent will my checkups be and what will they involve?
Are there any problems I should watch out for?
I would like to have a second opinion. Can you refer me to someone else?
Is my cancer hereditary?
What happens if I don't have treatment?
If I choose not to have treatment either now or in the future, what services are available to help me?
Will I still be able to have children?
Will I go through menopause?
If there are answers you do not understand, feel comfortable to say 'can you explain that again' or 'I am not sure what you mean by...'
Other questions and notes
It can be useful to jot down any other points you may want to discuss with your doctor.
Glossary
Most of the words lusted here are used by doctors and other health professionals who will be working with you.
ascites
A build up of fluid in the abdomen, making it swollen and bloated.
barium enema
A special x-ray of the bowel. Fluid is inserted into the bowel through the back passage (rectum) and x-rays are then taken.
benign
Not cancerous. Benign cells are not able to spread like cancer cells.
biopsy
The removal of a small sample of tissue from the body, for examination under a microscope, to help diagnose a disease.
CA 125/CEA
Tumour markers.
catheter
A flexible tube inserted into a narrow opening so that fluids can be introduced or removed.
cells
The 'building blocks' of the body. A human is made of millions of cells, which are adapted for different functions. Cells are able to reproduce themselves exactly, unless they are abnormal or damaged, as are cancer cells.
cervix
The lower part of the uterus, which protrudes into the vagina.
Chemotherapy
The use of special (cytotoxic) drugs to treat cancer by killing cancer cells or slowing their growth.
computerised tomography (CT) scan
The technique for constructing pictures of the body, by x-raying the part of the body to be examined from many different angles.
diagnosis
The process of finding out what a person's illness is by considering the person's signs and symptoms, medical background and results of diagnostic tests.
epithelium
The cells that make up the internal and external surfaces of the body, for example, skin, inside of lungs, ovaries.
Fallopian tubes
The tubes that carry the ova (eggs) from the ovary to the uterus. Each woman has two Fallopian tubes, one from each ovary.
genes
The tiny factors that govern the way the body's cells grow and behave. Each person has a set of many thousands of genes inherited from both parents. These genes are found in every cell of the body.
germ cells
Special cells in the ovary which can mature into ova (eggs).
gynaecological-oncologist
A doctor who specialises in treating women diagnosed with cancer of the reproductive organs.
hysterectomy
Surgical removal of the uterus.
inhibin
A tumour marker.
laparoscopy
A minor operation to allow the doctor to examine some of the organs in the lower abdomen and pelvis.
laparotomy
An operation in which a long cut is made in the abdomen.
lymph nodes
Also called lymph glands. Small, bean-shaped structures which form part of the lymphatic system. Lymph is the fluid that flows through this system and carries cells that help to fight disease and infection. The lymph nodes filter the lymph to remove bacteria and other harmful agents, such as cancer cells.
lymphoedema
Swelling caused by a build up of fluid. Can occur sometimes after lymph nodes have been removed.
malignant
Cancerous. Malignant cells can metastasise (spread) and can eventually cause death if they cannot be treated.
menopause
The natural cessation of menstruation (periods). This is the main event marking a woman's transition from when reproduction is possible to the post-reproductive years. Usually occurs between the ages of 45 and 55 years.
metastases
Also known as 'secondaries'. Tumours or masses of cells that develop when cancer cells break away from the primary (original) cancer and are carried by the lymphatic and blood systems to other parts of the body.
oestrogen
A female sex hormone mainly made by the ovaries.
omentum
A protective 'apron' of fatty tissue over the abdominal organs
osteoporosis
A condition that affects bones, making them thinner and weaker than normal and liable to fracture and break.
ova
the eggs which are released from the ovaries at ovulation, in readiness for fertilisation.
ovaries
The female sex organs which secrete important female hormones and contain the ova.
ovulation
The time in the menstrual cycle when ova are released from the ovary.
paracentesis
A procedure to drain away excess fluid from the abdomen.
pelvis/pelvic
The lower part of the trunk of the body: roughly, the area that extends from hip to hip and waist to groin.
pleural effusion
Collection of excess fluid in the lining of the lungs. This fluid can be drained away by a procedure called a pleural aspiration or a pleural tap.
progesterone
A hormone produced by the ovary that prepares the inner lining of the womb for pregnancy.
prognosis
An assessment of the future course and outcome of a person's disease.
radiotherapy
The use of radiation, usually x-rays or gamma rays, to kill cancer cells or injure them so they cannot grow and multiply. Radiotherapy treatment can also harm normal cells, but they are able to repair themselves.
sex-cord stromal cells
Cells of the ovary which release the female hormones.
tumour
A new or abnormal growth of tissue on or in the body.
tumour marker
A substance which, if found in a blood or tissue sample, suggests there may be a tumour present in the body.
ultrasound
'Ultrasound' is sound waves of a very high frequency (higher than the human ear can hear). If ultrasound is directed at the body, it is reflected back differently by different types of tissue. In an ultrasound scan, these differences are measured and used to build up pictures of structures in the body. Ultrasound pictures are usually taken by an ultrasound technician, who guides the scanning by watching the images on a screen like a television. The pictures that he or she records will be given to a specialist who will prepare a report which your own doctor will discuss with you.