
1. Introduction
This information has been prepared to help you understand more about cervical cancer (cancer of the cervix).
Many women feel understandably shocked and upset when they are told that they have or may have cervical cancer. This booklet is intended to help you to understand the diagnosis and treatment of cervical cancer. We also include information about available support services. We cannot advise you about the best treatment for you. You need to discuss this with your doctors. However, we hope this information will answer some of your questions and help you think about the questions you want to ask your doctors.
What is Cancer?
Cancer is a disease of the body’s cells. It starts in our genes. Our bodies are constantly making new cells; to enable us to grow, to replace worn out cells, or to heal damaged cells after an injury. Certain genes control this process. All cancers are caused by damage to these genes. This damage usually happens during our lifetime, although a small number of people inherit a damaged gene from a parent when they are born. Normally, cells grow and multiply in an orderly way. However, damaged genes can cause them to behave abnormally. They may grow into a lump, which is called a tumour. Tumours can be benign (not cancerous) or malignant (cancerous).
Benign tumours do not spread outside their normal boundary to other parts of the body. A malignant tumour is made up of cancer cells. When it first develops, this malignant tumour may be confined to its original site, a cancer in situ (or carcinoma in situ).
What is Cancer?
Cancer is a disease of the body’s cells. It starts in our genes. Our bodies are constantly making new cells; to enable us to grow, to replace worn out cells, or to heal damaged cells after an injury. Certain genes control this process. All cancers are caused by damage to these genes. This damage usually happens during our lifetime, although a small number of people inherit a damaged gene from a parent when they are born. Normally, cells grow and multiply in an orderly way. However, damaged genes can cause them to behave abnormally. They may grow into a lump, which is called a tumour.
Tumours can be benign (not cancerous) or malignant (cancerous).
Benign tumours do not spread outside their normal boundary to other parts of the body.
A malignant tumour is made up of cancer cells. When it first develops, this malignant tumour may be confined to its original site, a cancer in situ (or carcinoma in situ).
HOW CANCER SPREADS
If left untreated they may spread beyond their normal boundaries and into surrounding tissues (invasive cancer).
For a cancer to grow bigger than the head of a pin, it must grow its own blood vessels. This is called angiogenesis. Sometimes cells move away from the original (primary) cancer and invade other organs. When these cells reach a new site they may continue to grow and form another tumour at that site. This is called a secondary cancer or metastasis. In some cancers, it is the body's blood cells, which multiply abnormally. These cancers are called leukaemia, myeloma and lymphoma.
The Cervix
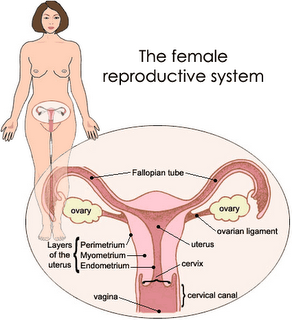
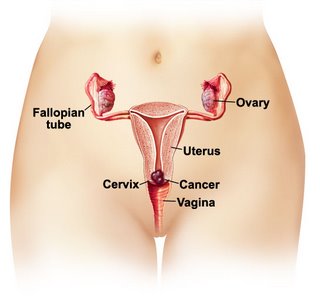
The cervix is at the lower part of the uterus (womb), which protrudes into the vagina. The cervix is sometimes called the neck of the womb. There is a small opening in the cervix, the cervical canal, which leads through the cervix into the main part of the uterus. The cervix has several important functions. It produces some of the moistness that helps lubricate the vagina. It also produces the mucus that helps sperm travel up to the Fallopian tubes in an effort to fertilise an egg from the ovary. The cervix holds the developing baby in the uterus during a pregnancy. During labour the cervix opens to allow the baby to be born.
The cervix is covered by two different kinds of cells. Squamous cells cover the outer part.
Cervix Endocervical cells cover the inner part.
Cervical cell abnormalities
Cervical cancer develops in stages. This is why regular Pap tests are so valuable: they can detect abnormal cells that may one day become cancerous.
Atypia
Atypia refers to minor changes to the cells, which can be detected in a Pap test. These changes may worsen or return to normal. If a Pap test picks up atypical changes, the woman will be advised to have another test in six months to see whether the changes have disappeared.
Dysplasia (also known as CIN or SIL)
Dysplasia is a type of abnormal change in the cells of the cervix. It is also called cervical intraepithelial neoplasia (CIN) and squamous intraepitheliallesion (SIL). CIN is graded into CIN I CIN II and CIN III, that is, mild, moderate and severe cervical cell changes. These conditions are not cancer but could later develop into cancer if left untreated; the term carcinoma in situ is sometimes still used to describe abnormal cell changes in the cervix. It is the same as CIN III.
Cervical cancer
There are two main types of cervical cancer. These are squamous cell carcinoma and adenocarcinoma. Squamous cell carcinoma, the most common type of cervical cancer, starts in the squamous or skin-like cells of the cervix. Adenocarcinoma is a less common type of cervical cancer. It starts in the glandular cells. In addition cervical cancer may be either microinvasive or invasive.
Microinvasive cervical cancer
This is when cancer cells have just broken through the bottom layer of the skin of the cervix. At this stage, the cells have not spread more than five millimetres into the tissues of the cervix.
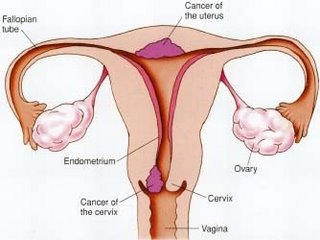
Invasive cervical cancer
In this, the cancer cells have spread from the surface skin of the cervix into the deeper tissues of the cervix. The cancer may also have spread to part of the vagina or to the lymph nodes and other tissues surrounding the cervix, within the pelvis, or beyond the genital and pelvic areas into nearby organs.
How common is cervical cancer?
In Malaysia each year approximately 1060 women are diagnosed with cervical cancer. Generally, cervical cancer takes a long time to develop and this is one reason why it is more common in women over the age of 40. However, as with all types of cancer, cervical cancer occasionally develops very quickly and is sometimes diagnosed in younger women.
Causes of cervical cancer
Some factors seem to put some women at a higher risk. These include:
· Human Papilloma or wart virus (HPV). Almost everyone is infected with HPV at some stage in his or her life. Most cases of HPV resolve themselves and have no ill effects. Many women have HPV and don't ever show signs of abnormal cell changes. The exact link between HPV infection and cervical cancer is unclear. It remains the subject of research.
· Daughters of women who used the drug diethylstilboestrol (DES) during pregnancy to prevent a miscarriage. The use of this drug has declined since the 1940s and 1950s.
· Smoking, which increases the risk of cervical cancer fourfold.
Colposcopy
Colposcopy gives a magnified view of the cervix. It uses an instrument called a colposcope, which is like a microscope on a stand. As with a Pap test, the doctor puts a speculum into your vagina to hold the walls slightly apart.
A colposcopy can be done in the doctor's room and takes only a few minutes. The specialist looks at your cervix through the colposcope. The doctor may coat the cervix with an iodine solution. This causes healthy cells to turn brown and abnormal cells to turn white. Some colposcopes have a special TV screen so you can watch the procedure if you wish.
If you are pregnant a colposcopy is quite safe. However, you should always tell your doctor if you are or think you may be pregnant as this may mean you would need different treatment. Sometimes it is necessary to have a punch or target biopsy taken at the same time.
Punch or target biopsy
In a punch or target biopsy, a small piece of tissue is removed with a special instrument and sent to a laboratory for examination. The doctor uses the colposcope to see the area that needs to be removed. You may feel a little pain when the biopsy is taken: ask the doctor to tell you when this might happen.
To allow your cervix to heal after a punch biopsy, your specialist will advise you about whether and for how long you should avoid sexual intercourse and the use of tampons. A punch or target biopsy can cause some bleeding or other discharge, but it will usually heal quickly. Women also often experience some pain afterwards, similar to menstrual cramping, which can be relieved with painkillers.
No definite diagnosis can usually be made until the results of the biopsy are received. This may take several days, sometimes longer.
Cone biopsy
If the punch or target biopsy shows abnormal cells on the surface of the cervix, it may be necessary to have a cone biopsy, which removes a larger and deeper area of tissue from the cervix. (It is called a cone biopsy because a cone-shaped area of tissue is taken from the inner base of the cervix). Sometimes this procedure removes all of the abnormal cells and no further treatment is needed. In other cases, it shows that the cells have spread into the cervix, and further treatment will be necessary.
You will have a general anaesthetic. You may be treated as a day patient or stay overnight in hospital. You may have some bleeding or cramping for a short while after the cone biopsy. Sexual intercourse and tampons should be avoided for two to three weeks. This allows time for your cervix to heal. Most women do not experience any problems after a cone biopsy, although occasionally some women have difficulty with their periods.
Your cervix will be weaker after a cone biopsy. You can still become pregnant but may be at more risk of having a miscarriage. Having some supportive stitches put in early in the pregnancy can help this; these stitches are removed before the baby is due. If you want to become pregnant in the future, you should discuss this and possible side effects with your doctor before you have a cone biopsy.
Cystoscopy and proctosigmoidoscopy
These procedures are done while you are under anaesthetic. They check whether the cancer has spread to other organs in your abdomen. A cystoscope is a thin, lighted instrument that is used to examine your bladder. A proctosigmoidoscope is a thin-lighted instrument that is used to examine the rectum and lower part of the large intestine.
Intravenous pyelogram (IVP)
This is an x-ray of your kidneys, bladder and ureters (the tubes that connect the kidneys to the bladder). An IVP can be done in hospital x-ray department or at a special clinic. You may be asked to go on a low fibre diet and take something to help empty your bowels before you have the IVP. Before the test, a dye that shows up on x-ray is injected into a vein in your arm. This dye concentrates in your kidneys, ureters and bladder so that the x-rays can show any problems. An IVP should not cause any side effects. Instead of an IVP, some specialists may recommend that you have an ultrasound to check your kidneys.
CT scan
A computerised tomography (CT) scan is usually done at a hospital or a special clinic. You do not need to be admitted to hospital and you should have no side effects. In a CT scan, x-rays are taken at different positions. This allows a two and three-dimensional image of the body to be built up.
Before the scan you will be asked to drink some fluid that shows up on x-rays. This makes it easier for abnormalities to be detected. You may also be asked to put a tampon into your vagina before the scan; this also makes it easier to detect any problems.
Magnetic resonance imaging
This test is similar to a CT scan but it uses magnetic fields instead of x-rays to build up a series of very clear and detailed images.
Other tests
You may be admitted to hospital, usually as a day patient, for an extensive physical examination. While you are under anaesthetic, your gynaecological oncologist will examine your bladder, bowel, vagina and pelvic area very carefully. A punch biopsy of your cervix may also be performed at this time.
Blood and urine tests are also usually done.
Treatment for dysplasia
If you are diagnosed with dysplasia, you may need treatment to remove the abnormal cells from the cervix.
In mild cases, all that may be needed is regular Pap tests. In more severe cases, the abnormal cells may be removed using cryosurgery (freezing), cauterisation (burning) or laser surgery. These procedures destroy the abnormal cells without harming normal tissue. A punch or cone biopsy may also remove all the abnormal cells.
Treatment for microinvasive cancer is usually by cone biopsy, although hysterectomy may occasionally be required. These treatments can cause temporary cramping or other pain, bleeding or a watery discharge. Although it is not cervical cancer, the diagnosis and treatment of dysplasia may still be a shock and it may take you some time to recover emotionally. Talking with friends, partners or relatives may help.
3. Treatment of cervical cancer
Once all your test results are available, your doctor will be able to discuss with you the best treatment for you. Sometimes there will be a choice or combination of treatments. The types or choices of treatment will vary with different women. This depends on whether the cancer is at an early stage or has spread, your age and general health. It is important to understand what the treatments will involve so that you can make the best decision for you. You may have a lot of questions to ask your doctor at this stage. Making a list can help you remember them. Treatments for cervical cancer include surgery, radiotherapy, chemotherapy or a combination of
these treatment
Cone biopsy
As discussed earlier, some very early cervical cancers may be treated with cone biopsy. However, great care is needed to ensure that all the cancer cells are removed, so the margins of the tissue removed are carefully examined. Most women who have a cone biopsy will not have any long-term side effects.
Lymph node dissection
This is also known as lymphadanectomy. It is a surgical procedure in which some lymph nodes near the site of the cancer are removed and examined to see if they contain cancer cells. Lymph node removal is usually performed at the time of radical hysterectomy. Leg swelling (lymphoedema) may result. Talk with your doctor about this.
Hysterectomy
A hysterectomy is the removal of the uterus by surgery. There are two kinds of hysterectomy. In a total hysterectomy, the uterus including the cervix is removed. In a radical hysterectomy, the cervix, support ligaments and top part of the vagina are removed. The ovaries are usually not removed in women who are still having periods. Lymph node dissection may also be done during a radical hysterectomy for cervical cancer.
For both types of hysterectomy, you will need a general anaesthetic. A radical hysterectomy is a longer operation and it may take you longer to recover. When you wake up from the operation, you will find that you have several tubes in place. You will have an intravenous drip which will give you fluid and drugs. Sometimes you may have a drain tube in your pelvis for a little while. You will also have a catheter inserted into your bladder to drain away urine. As you improve after the operation, these tubes will gradually be removed.
After the operation
As with all major operations, you will have some discomfort or pain. Painkillers can be taken to control this. They may be given through an intravenous drip or through an epidural tube into your spine. The epidural pain relief is similar to that given to women during childbirth. Let the doctor or nurse know when you are starting to feel uncomfortable--don't wait until the pain becomes severe.
A hysterectomy is a major operation. You may be in hospital for five to seven days for a total hysterectomy. If you have a radical hysterectomy you will need to be in hospital for about seven days. Your recovery time will depend on different factors. Don't expect to get back to your normal activities too quickly. For some women, it may take six weeks or even longer. During this time heavy work or lifting should be avoided. It may take some time before you feel completely well.
Before you go home from hospital, discuss with your doctor about what you can do and what you should avoid for a while, for example, when you can start to be sexually active again. There are many books about hysterectomy, which may be helpful.
Side effects of treatment for cervical cancer are also discussed.
Radiotherapy
Radiotherapy is the use of radiation to destroy cancer cells. Radiotherapy may be advised if you are not well enough for a major operation. It may also be advised if the tumour has spread into the tissues around the cervix, as this would be difficult to sure by surgery alone. Radiotherapy may also be used after surgery or combined with chemotherapy. Radiotherapy can be given in two ways: from outside or onside the body. In external radiotherapy, the radiation is directed from a machine at the cancer and surrounding tissue. In internal radiotherapy, radioactive material is put in thin tubes into your body, on or near the cancer. Usually both external and internal radiotherapy is used to treat cervical cancer.
If radiotherapy is advised, a doctor who specialises in radiotherapy treatment for women with cervical cancer will treat you. This doctor works closely with your gynaecological oncologist.
External radiotherapy
In external radiotherapy, special rays from a large machine are directed at the part of the body needing treatment. For women with cervical cancer, this is the pelvic area. Radiotherapy is usually given as an outpatient, five days a week for four to six weeks. The actual treatment takes two to three minutes each time. However the waiting and preparation time is longer. Like a normal x-ray, radiotherapy does not cause pain or discomfort as it is being given.
Currently, chemotherapy is given once a week with the external radiation.
Internal radiotherapy
In internal radiotherapy, a radioactive implant is placed inside your body as close to the tumour as possible. You will be given a general anaesthetic so that the implant can be inserted through your vagina. You will need to be admitted to hospital for a few days. The implant is left in place for up to 72 hours. The exact dose of radiotherapy given and the length of time the implant is left in position are very carefully measured.
You will be in a room of your own while the implant is in place. This is because the implant is radioactive. Some pre- cautions will need to be taken by the hospital staff as well as by your family to protect themselves from unnecessary radiation. The nursing staff will explain these precautions to you and your family before the implant is inserted. Make sure that you and your family understand what you need to do.
Side effects of radiotherapy
Radiotherapy may cause a number of side effects that are temporary and can be controlled. These include tiredness, depression, loss of appetite, diarrhoea, pain when passing urine and skin problems. The skin between your buttocks may feel sore, like the feeling you get from sunburn. Special cream can be used to relieve this burning feeling. If you have not been through menopause, radiotherapy will affect your ovaries and reduce their ability to produce normal hormones. This may cause infertility and symptoms of menopause.
When undergoing radiotherapy, you should allow plenty of time to rest. Remember to drink lots of water and have small but frequent meals. Ask the doctor or nurse about how to manage any side effects.
Chemotherapy
Chemotherapy is the treatment of cancer using anti-cancer drugs. The aim is to kill cancer cells while doing the least possible damage to normal cells. The drugs work by stopping the cancer cells from growing and reproducing.
Chemotherapy is usually given to women with more advanced cervical cancer or together with radiotherapy. Chemotherapy is usually given through a vein. You may need to stay in hospital overnight or you may be treated as a day patient. This depends on the drugs you are given and how you are feeling. A number of chemotherapy treatments, usually six, may be given every three to four weeks over several months. This depends on the disease and other treatments being used. Blood tests are taken before your next treatment to make sure your body's normal cells have had time to recover.
Side effects of chemotherapy
The side effects of chemotherapy vary according to the particular drugs used. They may include feeling sick, vomiting, depression, feeling off colour and tired, and some thinning or loss of hair from your body and head. These side effects are temporary, and measures can be taken to prevent or reduce them. Chemotherapy may also cause a temporary suspension of menstruation, or premature menopause.
Combined radiotherapy and chemotherapy
A combination of radiotherapy and chemotherapy is being used increasingly to treat cervical cancer. US trials found recently that women with invasive cervical cancer have better rates of survival when they receive chemotherapy that includes the drug cisplatin along with radiotherapy. Combined radiotherapy and chemotherapy causes more severe side effects than radiotherapy alone. The side effects include leucopoenia, nausea and vomiting. These effects are temporary and can be relieved.
Palliative treatment
If the cancer has spread and it is not possible to cure it, then your doctor will discuss various treatments for specific problems caused by the cancer. Palliative treatment is treatment that relieves or soothes pain and other symptoms of illness. Palliative care is available for all people who experience pain and distress associated with cancer, whatever their stage of cancer treatment. It is a particularly important type of treatment for people with advanced cancer, who cannot be cured but can expect to live without undue pain and distress. Palliative care includes pain relief using painkilling drugs and other measures. Pain is usually well controlled with oral medication. If pain is particularly severe or difficult to control, then you may have injections of pain-relieving medication.
General practitioners, specialists and specialist palliative care teams in hospital all play important roles in palliative treatment for people with early and advanced cancer. For further information contact The Resource and Wellness Centre.
Prognosis/ outlook
Cervical cancer can be effectively treated when it is found early. The vast majority of women with early cervical cancer will be cured. For women with more advanced disease, a cure may still be possible. For other women treatment can keep the disease under control for long periods of time.
For information about your own prognosis, you should talk with your doctor who is familiar with your full medical history. Even if your cancer is curable you may find that you often need reassurance from your specialist. This is normal as you may feel that you can no longer trust your body. Over time you will find that your confidence builds up again.
Making decisions about treatment
Sometimes it is difficult to make decisions about what is the right treatment for you. You may feel that everything is happening so fast that you do not have time to think things through. Some people find that waiting for test results and for treatment to begin is very difficult. While some women feel they are overwhelmed with information, others may feel that they don’t have enough. You need to make sure that you understand enough about your illness, the treatment and its side effects to make your decisions. Don’t be hurried into making a decision. Waiting a few extra days will not make a difference to the success of your treatment.
If you are offered a choice of treatments, you will need to weigh the advantages and disadvantages of each treatment. If only one type of treatment is recommended, ask your doctor to explain why other treatment choices are not advised. For the majority of women, cervical cancer can be cured. However, treatment may make it more difficult or impossible for you to become pregnant. This may be a blow for many women even if they already have a family. For other women who have not yet had children, it can be particularly hard. Taking time over your decisions is even more important in this situation.
For a few women with more advanced cervical cancer, treatment may be aimed at controlling symptoms rather than curing the cancer. Some women in this situation will choose treatment, even if it only offers a small chance of cure. Others want to make sure that the benefits of treatment will outweigh any side effects. Still others will choose the treatment they consider offers them the best quality of life.
Talking with doctors
You may want to see your doctor a few times before making a final decision on treatment. It is often difficult to take everything in, and you may need to ask the same questions more than once. You always have the right to find out what a suggested treatment means for you and the right to accept or refuse it. Before you see the doctor, it may help to write down your questions. At the end of this there is a list of questions that may assist you. Taking notes during the session can also help. Many people like to have a family member or friend go with them, to take part in the discussion, take notes, or simply listen. Some people find it is helpful to tape record the discussion.
Talking with others
Once you have discussed treatment options with your doctor, you may want to talk them over with family or friends, nursing staff, the hospital social worker or your own religious or spiritual adviser. Talking it over can help to sort out what course of action is right for you. The Resource and Wellness Centre has counsellors available to talk to people who telephone, and they can refer you to other sources of information and help. Telephone 03 2698 7300 or email contact@cancer.org.my
A second opinion
You may want to ask for a second opinion from another specialist This is understandable and may be a valuable part of your decision making process Your specialist or local doctor can refer you to another specialist and you can ask for your records to be sent to the second opinion doctor You can still ask for a second opinion even if you have already started treatment or still want to be treated by your first specialist.
Taking part in a clinical trial
Your doctor may suggest that you consider taking part in a clinical trial. Clinical trials are a vital part of the search to find better treatments for cancer. Doctors conduct clinical trials to test new or modify treatments and see if they are better than existing treatments. Many people all over the world have taken part in clinical trials that have resulted in improvements to cancer treatment. However, the decision to take part in a clinical trial is always yours.
If your doctor asks you to take part in a clinical trial, make sure that you fully understand the reasons for the trial and what it means for you. Before deciding whether or not to join the trial, you may wish to ask your doctor:
· What treatments are being tested and why?
· What tests are involved?
· What are the possible risks or side effects?
· How long will the trial last?
· Will I need to go into hospital for treatment?
· What will I do if any problems occur while I am in the trial?
If you decide to join a randomised clinical trial, you will be given the best existing treatment or a promising treatment. You will be chosen at random to receive one treatment or other, but it will always be at least the best treatment available. If you do join the clinical trial, you have the right to withdraw at any time, doing so will not jeopardise your treatment for cancer. It is always your decision to take part in a clinical trial. If you do not want to take part, your doctor will discuss the best current treatment choices with you.
Recovery and follow-up care
After the completion of your treatment, you will need to have regular checkups. Your doctor will decide how often you will need checkups, as everyone is different. They will gradually become less frequent if you have no further problems. If the disease flares up, or relapses, it can often be treated successfully. The treatment used for the relapse is often different from the first treatment.
4. Seeking Support
It is normal to feel a range of intense emotions for some time after your diagnosis and treatment. You may feel sad, depressed, angry or frustrated. It is important to acknowledge these reactions and understand that it may take some time before you feel well again. It may be helpful to talk about your feelings with your partner, family members or friends, or with a hospital counsellor, social worker, psychologist or your religious or spiritual adviser. Sometimes you may find that your friends and family do not know what to say to you: they may have difficulty with their feelings as well. Some people may feel so uncomfortable that they avoid you. They may expect you to ‘lead the way’ and tell them what you need. You may prefer to ask a close family member or a friend to talk with other people for you.
Loss of fertility can be difficult for many women to cope with, even if they already have a child or children, or have chosen not to have children. You, with or without your partner, may need to seek help to cope with your grief. This may be through a social worker, psychologist and psychiatrist or through other support services. Permanent care or adoption of a child may be a choice for some women. This requires dedication and perseverance and not all couples who wish to adopt a child are able to do so.
Diet
A balanced, nutritious diet will help you keep as well as possible and cope with the cancer and any side effects treatment. Depending on the kind of treatment you have had, you may have special dietary needs. A dietician may help plan the best foods for your particular situation; ones that you find tempting, easy to eat and nutritious. The Resource and Wellness Centre have a resident dietician. To make an appointment please call 03 2698 7300 or email contact@cancer.org.my
Exercise
You will probably find it helpful to stay active and to exercise regularly if you can. The amount and type of exercise you do will depend upon what you are used to and how well you feel.
Discuss with your doctor what is likely to be best for you.
Relaxation techniques
Some women find relaxation or meditation techniques helpful. The Resource and Wellness Centre conduct relaxation and meditation classes.
Sexuality and cancer
The diagnosis and treatment of cervical cancer may affect how you feel about yourself and your relationships. It is a time when you will need support as your relationships may change. Current or new partners may also have difficulty adjusting and may need reassurance. You may find it helpful to share your feelings with each other. However, this is not always possible as with all crises, some relationships suffer under the strain. You may both need to seek separate support.
If you need radiotherapy you are usually able to continue being sexually active during treatment, as long as it is comfortable for you and you feel like it. Everyone is different and you should be guided by how you feel. You may find that, particularly near the end of treatment, you don't feel like penetrative sex. If you have vaginal dryness, a gel such as KY Jelly can be helpful. This can be bought from a chemist or supermarket. Some women may bleed after sexual intercourse when they are having radiotherapy. Don't be worried but let your doctor or nurse know
After you have had your check-up following surgery you will be able to recommence sexual activity. However, some women find that it takes time before they feel both physically and emotionally well enough. It may be some time until you feel you are ready for sex. You may need to build up your confidence first. Sharing affection with your partner through kissing, caressing and touching can give you both much pleasure. Talking about your needs together is important to help you feel more confident and to reduce any fears.
If you are resuming vaginal intercourse, you may wish to proceed slowly. As your vagina may be a little shorter after treatment, you may find it better to try different positions for intercourse. You may want to choose a position where you have more control and there is less pressure to your pelvic area. If you have difficulty you may need expert advice.
If there are some special aids to help you gradually stretch your vagina after surgery or radiotherapy. These are called vaginal dilators and are available from your gynaecological oncologist or from specialist services like family planning clinics. If you find that you are having difficulty resuming your sexual relationship, you may need specialist help and advice. You may want to talk with your doctor about this or ask for advice on where you can get help. Remember, it is normal not to feel like sex after being treated for cancer.
Coping with side effects
It may take some time to recover from the various types of treatment. You will find that there are physical changes as well as many emotional changes to cope with. It is important that you, your partner, family and employer are prepared for this.
Premature menopause
Ovaries produce the hormones oestrogen and progesterone. If your ovaries are surgically removed or damaged by radiotherapy, they will no longer produce these hormones. This means that you will have premature menopause. Your body will have lower levels of these hormones circulating in the blood, which can cause symptoms such as hot flushes and palpitations. Oestrogen s an important protection against osteoporosis and heart disease, so premature menopause may increase your risk of these diseases.
Hormone replacement therapy (HRT) can be taken to reduce or prevent symptoms of menopause. HRT is a combination of oestrogen and progesterone, taken in tablets. You will need to discuss with your doctor, and evaluate for yourself, the benefits and possible risks of taking HRT. There are also many useful books about menopause, which may help you with your decisions.
Bladder problems
Bladder sensations or control may change after treatment. Some women find they need to go to the toilet more often; others find that they need to go in a hurry and sometimes don't get there in time. Others find that they pass urine when they cough or sneeze. While these problems may improve, even a small loss of bladder control can be upsetting. If bladder control is a problem for you, you should seek help. Your specialist will be able to suggest ways to help with bladder control. These may include special exercises to strengthen the muscles of your pelvic floor. You should also be visited in hospital by a physiotherapist who can teach you about these exercises, or you can contact The Resource and Wellness Centre.
Bowel problems
After surgery some women may have problems with their bowels for a while. This may be wind pain that can be helped by sucking strong peppermints. Other women find that they become constipated or suffer from diarrhoea and may need to make adjustments to their diet or take medication. Talk with your doctor if your bowel problems or pain do not improve.
Lymphoedema
Lymphoedema is swelling of part of the body, usually the legs or arms. It may occur after treatment for cervical cancer if you have had the lymph nodes in your pelvis removed (a lymphadenectomy). Removal of the nodes may prevent normal draining of the fluid from the legs. As a result fluid can build up in one or both legs causing swelling. This usually does not occur until some time after the original treatment.
It is not possible to predict whether you will have problems with lymphoedema. If you begin to have problems seek immediate help, as symptoms are better managed if treated early. Seek advice from your specialist or nurse. You may be given special stockings to wear after your operation.
Some hospitals have specialist physiotherapists who can advise you on how you may be able to reduce your risk of developing lymphoedema. They also help you if lymphoedema does occur in the future. For further information about lymphoedema, contact the Resource and Wellness Centre.
Cancer support groups
Cancer support groups offer mutual support and information to people with cancer and, often, to their families. It can help to talk with others who have gone through the same experience. Support groups can also offer many practical suggestions and ways of coping. For information about the Support Groups, contact the Resource and Wellness Centre.
Caring for someone with cancer
Caring for someone with cancer can be very stressful; particularly when it is someone you care about very much. Look after yourself during this time. Give yourself some time out, and share your worries and concerns with someone outside. You may have to make many decisions. You will probably have to attend many appointments with doctors, support services and hospitals. Many people have found it helpful to take with them another member of the family or a close friend. It also helps to write down questions beforehand, and to take notes during the appointment.
Cancer support group membership is generally open to patients and carers. A support group can offer the chance to share experiences and ways of coping.
Cancer Information and Support Service
The Resource and Wellness Centre is a service of the National Cancer Society of Malaysia. It is a confidential service where you can talk about your concerns and needs with specially trained staff. The staff can send you written information and can put you in touch with appropriate services in your own area. Telephone 03 2698 7300 or email contact@cancer.org.my
5. Information Checklist
1 What type of cancer do I have?
2 How extensive is my cancer?
3 What treatment do you advise for my cancer and why?
4 Will my treatment (and surgery) be performed by a doctor who specialises in cervical cancer?
5 Are there other treatment choices for me? If not, why not?
6 What are the risks and possible side effects of each treatment?
7 Will I have to stay in hospital, or will I be treated as an out patient?
8 How long will the treatment take? How much will it affect what I can do?
9 How much will it cost?
10 Will I have a lot of pain with the operation? What will be done about this?
11 If I need further treatment, what will it be like and when will it begin?
12 Will the treatment affect my sexual relationships?
13 How frequent will my check-ups be and what will they involve?
14 Are there any problems I should watch out for?
15 I would like to have a second opinion. Can you refer me to someone else?
16 Is my cancer hereditary?
If there are answers you do not understand, feel comfortable to say 'can you explain that again' or 'I am not sure what you mean by ...'
Glossary
Most of the words listed here are used on this web page, others are words you are likely to hear used by doctors and other health professionals who will be working with you.
adenocarcinoma
A cancer that has arisen in glandular cells.
anaesthetic
A drug given to stop a person feeling pain. A 'local' anaesthetic numbs part of the body; a 'general' anaesthetic cause temporary loss of consciousness.
angiogenesis
The formation of new blood vessels to support tissue. Angiogenesis enables tumours to develop their own blood supply, which helps them to survive and grow.
benign
Not cancerous. Benign cells are not able to spread like cancer cells.
biopsy
The removal of a small sample of tissue from the body, for examination under a microscope, to help diagnose a disease.
carcinoma in situ
Cancer that involves only the cells in which it began and has not spread to nearby tissues.
catheter
A flexible tube inserted into a narrow opening so that fluids can be introduced or removed.
cells
The 'building blocks' of the body. A human is made of millions of cells, which are adapted for different functions. Cells are able
to reproduce themselves exactly, unless they are a abnormal or damaged, as are cancer cells.
cervix
The lower part of the uterus, which extends into the vagina
chemotherapy
The use of special (cytotoxic) drugs to treat cancer by killing cancer cells or slowing their growth.
colposcopy
The examination of the vagina and cervix with a magnifying instrument, called a colposcope, to check these tissues for abnormality.
computerised tomography (CT) scan
The technique for constructing pictures from cross sections of the body, by x-raying the part of the body to be examined from many different angles.
cone biopsy
The removal of a cone-shaped piece of the cervix. It may be used to both diagnose and treat a problem.
dysplasia
An alteration in size, shape and arrangement of normal cells. Dysplastic cells are abnormal but are not cancerous. They may progress into cancer.
endocervical cells
The cells lining the inside of the cervix.
genes
The tiny factors that govern the way the body's cells grow and behave. Each person has a set of many thousands of genes inherited from both parents. These genes are found in every cell of the body.
gynaecological oncologist
A doctor who specialises in treating women diagnosed with cancer of the reproductive organs.
hormone replacement therapy (HRT)
Female hormones (oestrogen and progesterone) which can be taken by women to relieve symptoms of menopause.
hysterectomy
The removal of a woman's uterus by surgery.
intravenous
Into a vein. An intravenous drip gives drugs directly into a vein.
leucopoenia
A reduction in the number of white blood cells in the blood
lymphadenectomy
Removal of the lymph nodes from a particular part of the body
lymph nodes
Also called lymph glands. Small, bean-shaped structures which form part of the lymphatic system. Lymph is the fluid that flows through this system and carries cells that help to fight disease and infection. The lymph nodes filter the lymph to remove bacteria and other harmful agents, such as cancer cells.
lymph vesselS
Part of the lymphatic system. The lymphatic system is part of the immune system, which protects the body against ‘invaders’, like bacteria and parasites. The lymphatic system is a network of small lymph nodes connected by very thin lymph vessels, which branch into every part of the body.
lymphoedema
Swelling of a part of the body, usually the legs or arms. Caused by the blockage or removal of the lymph nodes so causing fluid (lymph) to accumulate.
malignant
Cancerous. Malignant cells can spread (metastasise) and can eventually cause death if they cannot be treated.
menopause
The natural cessation of a woman's periods or menstruation. This is the main event marking a woman's transition from when having children is possible to the post-reproductive years. Usually occurs between the ages of 45 and 55 years.
metastases
Also known as 'secondaries'. Tumours or masses of cells that develop when cancer cells break away from the original (primary) cancer and are carried by the lymphatic and blood systems to other parts of the body.
Pap test
A test that can detect changes in cervical cells. Some cells are scraped off the cervix and sent to a laboratory for examination under a microscope.
prognosis
An assessment of the course and likely outcome of a person's disease.
radiotherapy
The use of radiation to kill cancer cells. Radiation can be directed at a tumour from outside the body, or a radioactive source may be implanted into a tumour and the surrounding tissue.
squamous cell carcinoma
A cancer that arises in the squamous or skin-like cells of the cervix.
tumour
A new or abnormal growth of tissue on or in the body.
Ultrasound
‘Ultrasound’ is the sound waves of a very high frequency (higher than human can hear). If ultrasound is directed at the body it is reflected back differently by different types of the tissue. In an ultrasound scan, these differences are measures and used to build up pictures of structures in the body. Ultra sound pictures are usually taken by an ultrasound technician, who guides the scanning by watching the images on a screen like a television.
Note:
If you have or suspect you may have a health problem, you should consult your health care provider. We cannot advice you about the best treatment for you. You will need to discuss this with your own doctors. However, we hope this information will answer some of your questions and help you into thinking about questions you want to ask your doctors.
Many women feel understandably shocked and upset when they are told that they have or may have cervical cancer. This booklet is intended to help you to understand the diagnosis and treatment of cervical cancer. We also include information about available support services. We cannot advise you about the best treatment for you. You need to discuss this with your doctors. However, we hope this information will answer some of your questions and help you think about the questions you want to ask your doctors.
What is Cancer?
Cancer is a disease of the body’s cells. It starts in our genes. Our bodies are constantly making new cells; to enable us to grow, to replace worn out cells, or to heal damaged cells after an injury. Certain genes control this process. All cancers are caused by damage to these genes. This damage usually happens during our lifetime, although a small number of people inherit a damaged gene from a parent when they are born. Normally, cells grow and multiply in an orderly way. However, damaged genes can cause them to behave abnormally. They may grow into a lump, which is called a tumour. Tumours can be benign (not cancerous) or malignant (cancerous).
Benign tumours do not spread outside their normal boundary to other parts of the body. A malignant tumour is made up of cancer cells. When it first develops, this malignant tumour may be confined to its original site, a cancer in situ (or carcinoma in situ).
What is Cancer?
Cancer is a disease of the body’s cells. It starts in our genes. Our bodies are constantly making new cells; to enable us to grow, to replace worn out cells, or to heal damaged cells after an injury. Certain genes control this process. All cancers are caused by damage to these genes. This damage usually happens during our lifetime, although a small number of people inherit a damaged gene from a parent when they are born. Normally, cells grow and multiply in an orderly way. However, damaged genes can cause them to behave abnormally. They may grow into a lump, which is called a tumour.
Tumours can be benign (not cancerous) or malignant (cancerous).
Benign tumours do not spread outside their normal boundary to other parts of the body.
A malignant tumour is made up of cancer cells. When it first develops, this malignant tumour may be confined to its original site, a cancer in situ (or carcinoma in situ).
HOW CANCER SPREADS
If left untreated they may spread beyond their normal boundaries and into surrounding tissues (invasive cancer).
For a cancer to grow bigger than the head of a pin, it must grow its own blood vessels. This is called angiogenesis. Sometimes cells move away from the original (primary) cancer and invade other organs. When these cells reach a new site they may continue to grow and form another tumour at that site. This is called a secondary cancer or metastasis. In some cancers, it is the body's blood cells, which multiply abnormally. These cancers are called leukaemia, myeloma and lymphoma.
The Cervix
The cervix is at the lower part of the uterus (womb), which protrudes into the vagina. The cervix is sometimes called the neck of the womb. There is a small opening in the cervix, the cervical canal, which leads through the cervix into the main part of the uterus. The cervix has several important functions. It produces some of the moistness that helps lubricate the vagina. It also produces the mucus that helps sperm travel up to the Fallopian tubes in an effort to fertilise an egg from the ovary. The cervix holds the developing baby in the uterus during a pregnancy. During labour the cervix opens to allow the baby to be born.
The cervix is covered by two different kinds of cells. Squamous cells cover the outer part.
Cervix Endocervical cells cover the inner part.
Cervical cell abnormalities
Cervical cancer develops in stages. This is why regular Pap tests are so valuable: they can detect abnormal cells that may one day become cancerous.
Atypia
Atypia refers to minor changes to the cells, which can be detected in a Pap test. These changes may worsen or return to normal. If a Pap test picks up atypical changes, the woman will be advised to have another test in six months to see whether the changes have disappeared.
Dysplasia (also known as CIN or SIL)
Dysplasia is a type of abnormal change in the cells of the cervix. It is also called cervical intraepithelial neoplasia (CIN) and squamous intraepitheliallesion (SIL). CIN is graded into CIN I CIN II and CIN III, that is, mild, moderate and severe cervical cell changes. These conditions are not cancer but could later develop into cancer if left untreated; the term carcinoma in situ is sometimes still used to describe abnormal cell changes in the cervix. It is the same as CIN III.
Cervical cancer
There are two main types of cervical cancer. These are squamous cell carcinoma and adenocarcinoma. Squamous cell carcinoma, the most common type of cervical cancer, starts in the squamous or skin-like cells of the cervix. Adenocarcinoma is a less common type of cervical cancer. It starts in the glandular cells. In addition cervical cancer may be either microinvasive or invasive.
Microinvasive cervical cancer
This is when cancer cells have just broken through the bottom layer of the skin of the cervix. At this stage, the cells have not spread more than five millimetres into the tissues of the cervix.
Invasive cervical cancer
In this, the cancer cells have spread from the surface skin of the cervix into the deeper tissues of the cervix. The cancer may also have spread to part of the vagina or to the lymph nodes and other tissues surrounding the cervix, within the pelvis, or beyond the genital and pelvic areas into nearby organs.
How common is cervical cancer?
In Malaysia each year approximately 1060 women are diagnosed with cervical cancer. Generally, cervical cancer takes a long time to develop and this is one reason why it is more common in women over the age of 40. However, as with all types of cancer, cervical cancer occasionally develops very quickly and is sometimes diagnosed in younger women.
Causes of cervical cancer
Some factors seem to put some women at a higher risk. These include:
· Human Papilloma or wart virus (HPV). Almost everyone is infected with HPV at some stage in his or her life. Most cases of HPV resolve themselves and have no ill effects. Many women have HPV and don't ever show signs of abnormal cell changes. The exact link between HPV infection and cervical cancer is unclear. It remains the subject of research.
· Daughters of women who used the drug diethylstilboestrol (DES) during pregnancy to prevent a miscarriage. The use of this drug has declined since the 1940s and 1950s.
· Smoking, which increases the risk of cervical cancer fourfold.
Colposcopy
Colposcopy gives a magnified view of the cervix. It uses an instrument called a colposcope, which is like a microscope on a stand. As with a Pap test, the doctor puts a speculum into your vagina to hold the walls slightly apart.
A colposcopy can be done in the doctor's room and takes only a few minutes. The specialist looks at your cervix through the colposcope. The doctor may coat the cervix with an iodine solution. This causes healthy cells to turn brown and abnormal cells to turn white. Some colposcopes have a special TV screen so you can watch the procedure if you wish.
If you are pregnant a colposcopy is quite safe. However, you should always tell your doctor if you are or think you may be pregnant as this may mean you would need different treatment. Sometimes it is necessary to have a punch or target biopsy taken at the same time.
Punch or target biopsy
In a punch or target biopsy, a small piece of tissue is removed with a special instrument and sent to a laboratory for examination. The doctor uses the colposcope to see the area that needs to be removed. You may feel a little pain when the biopsy is taken: ask the doctor to tell you when this might happen.
To allow your cervix to heal after a punch biopsy, your specialist will advise you about whether and for how long you should avoid sexual intercourse and the use of tampons. A punch or target biopsy can cause some bleeding or other discharge, but it will usually heal quickly. Women also often experience some pain afterwards, similar to menstrual cramping, which can be relieved with painkillers.
No definite diagnosis can usually be made until the results of the biopsy are received. This may take several days, sometimes longer.
Cone biopsy
If the punch or target biopsy shows abnormal cells on the surface of the cervix, it may be necessary to have a cone biopsy, which removes a larger and deeper area of tissue from the cervix. (It is called a cone biopsy because a cone-shaped area of tissue is taken from the inner base of the cervix). Sometimes this procedure removes all of the abnormal cells and no further treatment is needed. In other cases, it shows that the cells have spread into the cervix, and further treatment will be necessary.
You will have a general anaesthetic. You may be treated as a day patient or stay overnight in hospital. You may have some bleeding or cramping for a short while after the cone biopsy. Sexual intercourse and tampons should be avoided for two to three weeks. This allows time for your cervix to heal. Most women do not experience any problems after a cone biopsy, although occasionally some women have difficulty with their periods.
Your cervix will be weaker after a cone biopsy. You can still become pregnant but may be at more risk of having a miscarriage. Having some supportive stitches put in early in the pregnancy can help this; these stitches are removed before the baby is due. If you want to become pregnant in the future, you should discuss this and possible side effects with your doctor before you have a cone biopsy.
Cystoscopy and proctosigmoidoscopy
These procedures are done while you are under anaesthetic. They check whether the cancer has spread to other organs in your abdomen. A cystoscope is a thin, lighted instrument that is used to examine your bladder. A proctosigmoidoscope is a thin-lighted instrument that is used to examine the rectum and lower part of the large intestine.
Intravenous pyelogram (IVP)
This is an x-ray of your kidneys, bladder and ureters (the tubes that connect the kidneys to the bladder). An IVP can be done in hospital x-ray department or at a special clinic. You may be asked to go on a low fibre diet and take something to help empty your bowels before you have the IVP. Before the test, a dye that shows up on x-ray is injected into a vein in your arm. This dye concentrates in your kidneys, ureters and bladder so that the x-rays can show any problems. An IVP should not cause any side effects. Instead of an IVP, some specialists may recommend that you have an ultrasound to check your kidneys.
CT scan
A computerised tomography (CT) scan is usually done at a hospital or a special clinic. You do not need to be admitted to hospital and you should have no side effects. In a CT scan, x-rays are taken at different positions. This allows a two and three-dimensional image of the body to be built up.
Before the scan you will be asked to drink some fluid that shows up on x-rays. This makes it easier for abnormalities to be detected. You may also be asked to put a tampon into your vagina before the scan; this also makes it easier to detect any problems.
Magnetic resonance imaging
This test is similar to a CT scan but it uses magnetic fields instead of x-rays to build up a series of very clear and detailed images.
Other tests
You may be admitted to hospital, usually as a day patient, for an extensive physical examination. While you are under anaesthetic, your gynaecological oncologist will examine your bladder, bowel, vagina and pelvic area very carefully. A punch biopsy of your cervix may also be performed at this time.
Blood and urine tests are also usually done.
Treatment for dysplasia
If you are diagnosed with dysplasia, you may need treatment to remove the abnormal cells from the cervix.
In mild cases, all that may be needed is regular Pap tests. In more severe cases, the abnormal cells may be removed using cryosurgery (freezing), cauterisation (burning) or laser surgery. These procedures destroy the abnormal cells without harming normal tissue. A punch or cone biopsy may also remove all the abnormal cells.
Treatment for microinvasive cancer is usually by cone biopsy, although hysterectomy may occasionally be required. These treatments can cause temporary cramping or other pain, bleeding or a watery discharge. Although it is not cervical cancer, the diagnosis and treatment of dysplasia may still be a shock and it may take you some time to recover emotionally. Talking with friends, partners or relatives may help.
3. Treatment of cervical cancer
Once all your test results are available, your doctor will be able to discuss with you the best treatment for you. Sometimes there will be a choice or combination of treatments. The types or choices of treatment will vary with different women. This depends on whether the cancer is at an early stage or has spread, your age and general health. It is important to understand what the treatments will involve so that you can make the best decision for you. You may have a lot of questions to ask your doctor at this stage. Making a list can help you remember them. Treatments for cervical cancer include surgery, radiotherapy, chemotherapy or a combination of
these treatment
Cone biopsy
As discussed earlier, some very early cervical cancers may be treated with cone biopsy. However, great care is needed to ensure that all the cancer cells are removed, so the margins of the tissue removed are carefully examined. Most women who have a cone biopsy will not have any long-term side effects.
Lymph node dissection
This is also known as lymphadanectomy. It is a surgical procedure in which some lymph nodes near the site of the cancer are removed and examined to see if they contain cancer cells. Lymph node removal is usually performed at the time of radical hysterectomy. Leg swelling (lymphoedema) may result. Talk with your doctor about this.
Hysterectomy
A hysterectomy is the removal of the uterus by surgery. There are two kinds of hysterectomy. In a total hysterectomy, the uterus including the cervix is removed. In a radical hysterectomy, the cervix, support ligaments and top part of the vagina are removed. The ovaries are usually not removed in women who are still having periods. Lymph node dissection may also be done during a radical hysterectomy for cervical cancer.
For both types of hysterectomy, you will need a general anaesthetic. A radical hysterectomy is a longer operation and it may take you longer to recover. When you wake up from the operation, you will find that you have several tubes in place. You will have an intravenous drip which will give you fluid and drugs. Sometimes you may have a drain tube in your pelvis for a little while. You will also have a catheter inserted into your bladder to drain away urine. As you improve after the operation, these tubes will gradually be removed.
After the operation
As with all major operations, you will have some discomfort or pain. Painkillers can be taken to control this. They may be given through an intravenous drip or through an epidural tube into your spine. The epidural pain relief is similar to that given to women during childbirth. Let the doctor or nurse know when you are starting to feel uncomfortable--don't wait until the pain becomes severe.
A hysterectomy is a major operation. You may be in hospital for five to seven days for a total hysterectomy. If you have a radical hysterectomy you will need to be in hospital for about seven days. Your recovery time will depend on different factors. Don't expect to get back to your normal activities too quickly. For some women, it may take six weeks or even longer. During this time heavy work or lifting should be avoided. It may take some time before you feel completely well.
Before you go home from hospital, discuss with your doctor about what you can do and what you should avoid for a while, for example, when you can start to be sexually active again. There are many books about hysterectomy, which may be helpful.
Side effects of treatment for cervical cancer are also discussed.
Radiotherapy
Radiotherapy is the use of radiation to destroy cancer cells. Radiotherapy may be advised if you are not well enough for a major operation. It may also be advised if the tumour has spread into the tissues around the cervix, as this would be difficult to sure by surgery alone. Radiotherapy may also be used after surgery or combined with chemotherapy. Radiotherapy can be given in two ways: from outside or onside the body. In external radiotherapy, the radiation is directed from a machine at the cancer and surrounding tissue. In internal radiotherapy, radioactive material is put in thin tubes into your body, on or near the cancer. Usually both external and internal radiotherapy is used to treat cervical cancer.
If radiotherapy is advised, a doctor who specialises in radiotherapy treatment for women with cervical cancer will treat you. This doctor works closely with your gynaecological oncologist.
External radiotherapy
In external radiotherapy, special rays from a large machine are directed at the part of the body needing treatment. For women with cervical cancer, this is the pelvic area. Radiotherapy is usually given as an outpatient, five days a week for four to six weeks. The actual treatment takes two to three minutes each time. However the waiting and preparation time is longer. Like a normal x-ray, radiotherapy does not cause pain or discomfort as it is being given.
Currently, chemotherapy is given once a week with the external radiation.
Internal radiotherapy
In internal radiotherapy, a radioactive implant is placed inside your body as close to the tumour as possible. You will be given a general anaesthetic so that the implant can be inserted through your vagina. You will need to be admitted to hospital for a few days. The implant is left in place for up to 72 hours. The exact dose of radiotherapy given and the length of time the implant is left in position are very carefully measured.
You will be in a room of your own while the implant is in place. This is because the implant is radioactive. Some pre- cautions will need to be taken by the hospital staff as well as by your family to protect themselves from unnecessary radiation. The nursing staff will explain these precautions to you and your family before the implant is inserted. Make sure that you and your family understand what you need to do.
Side effects of radiotherapy
Radiotherapy may cause a number of side effects that are temporary and can be controlled. These include tiredness, depression, loss of appetite, diarrhoea, pain when passing urine and skin problems. The skin between your buttocks may feel sore, like the feeling you get from sunburn. Special cream can be used to relieve this burning feeling. If you have not been through menopause, radiotherapy will affect your ovaries and reduce their ability to produce normal hormones. This may cause infertility and symptoms of menopause.
When undergoing radiotherapy, you should allow plenty of time to rest. Remember to drink lots of water and have small but frequent meals. Ask the doctor or nurse about how to manage any side effects.
Chemotherapy
Chemotherapy is the treatment of cancer using anti-cancer drugs. The aim is to kill cancer cells while doing the least possible damage to normal cells. The drugs work by stopping the cancer cells from growing and reproducing.
Chemotherapy is usually given to women with more advanced cervical cancer or together with radiotherapy. Chemotherapy is usually given through a vein. You may need to stay in hospital overnight or you may be treated as a day patient. This depends on the drugs you are given and how you are feeling. A number of chemotherapy treatments, usually six, may be given every three to four weeks over several months. This depends on the disease and other treatments being used. Blood tests are taken before your next treatment to make sure your body's normal cells have had time to recover.
Side effects of chemotherapy
The side effects of chemotherapy vary according to the particular drugs used. They may include feeling sick, vomiting, depression, feeling off colour and tired, and some thinning or loss of hair from your body and head. These side effects are temporary, and measures can be taken to prevent or reduce them. Chemotherapy may also cause a temporary suspension of menstruation, or premature menopause.
Combined radiotherapy and chemotherapy
A combination of radiotherapy and chemotherapy is being used increasingly to treat cervical cancer. US trials found recently that women with invasive cervical cancer have better rates of survival when they receive chemotherapy that includes the drug cisplatin along with radiotherapy. Combined radiotherapy and chemotherapy causes more severe side effects than radiotherapy alone. The side effects include leucopoenia, nausea and vomiting. These effects are temporary and can be relieved.
Palliative treatment
If the cancer has spread and it is not possible to cure it, then your doctor will discuss various treatments for specific problems caused by the cancer. Palliative treatment is treatment that relieves or soothes pain and other symptoms of illness. Palliative care is available for all people who experience pain and distress associated with cancer, whatever their stage of cancer treatment. It is a particularly important type of treatment for people with advanced cancer, who cannot be cured but can expect to live without undue pain and distress. Palliative care includes pain relief using painkilling drugs and other measures. Pain is usually well controlled with oral medication. If pain is particularly severe or difficult to control, then you may have injections of pain-relieving medication.
General practitioners, specialists and specialist palliative care teams in hospital all play important roles in palliative treatment for people with early and advanced cancer. For further information contact The Resource and Wellness Centre.
Prognosis/ outlook
Cervical cancer can be effectively treated when it is found early. The vast majority of women with early cervical cancer will be cured. For women with more advanced disease, a cure may still be possible. For other women treatment can keep the disease under control for long periods of time.
For information about your own prognosis, you should talk with your doctor who is familiar with your full medical history. Even if your cancer is curable you may find that you often need reassurance from your specialist. This is normal as you may feel that you can no longer trust your body. Over time you will find that your confidence builds up again.
Making decisions about treatment
Sometimes it is difficult to make decisions about what is the right treatment for you. You may feel that everything is happening so fast that you do not have time to think things through. Some people find that waiting for test results and for treatment to begin is very difficult. While some women feel they are overwhelmed with information, others may feel that they don’t have enough. You need to make sure that you understand enough about your illness, the treatment and its side effects to make your decisions. Don’t be hurried into making a decision. Waiting a few extra days will not make a difference to the success of your treatment.
If you are offered a choice of treatments, you will need to weigh the advantages and disadvantages of each treatment. If only one type of treatment is recommended, ask your doctor to explain why other treatment choices are not advised. For the majority of women, cervical cancer can be cured. However, treatment may make it more difficult or impossible for you to become pregnant. This may be a blow for many women even if they already have a family. For other women who have not yet had children, it can be particularly hard. Taking time over your decisions is even more important in this situation.
For a few women with more advanced cervical cancer, treatment may be aimed at controlling symptoms rather than curing the cancer. Some women in this situation will choose treatment, even if it only offers a small chance of cure. Others want to make sure that the benefits of treatment will outweigh any side effects. Still others will choose the treatment they consider offers them the best quality of life.
Talking with doctors
You may want to see your doctor a few times before making a final decision on treatment. It is often difficult to take everything in, and you may need to ask the same questions more than once. You always have the right to find out what a suggested treatment means for you and the right to accept or refuse it. Before you see the doctor, it may help to write down your questions. At the end of this there is a list of questions that may assist you. Taking notes during the session can also help. Many people like to have a family member or friend go with them, to take part in the discussion, take notes, or simply listen. Some people find it is helpful to tape record the discussion.
Talking with others
Once you have discussed treatment options with your doctor, you may want to talk them over with family or friends, nursing staff, the hospital social worker or your own religious or spiritual adviser. Talking it over can help to sort out what course of action is right for you. The Resource and Wellness Centre has counsellors available to talk to people who telephone, and they can refer you to other sources of information and help. Telephone 03 2698 7300 or email contact@cancer.org.my
A second opinion
You may want to ask for a second opinion from another specialist This is understandable and may be a valuable part of your decision making process Your specialist or local doctor can refer you to another specialist and you can ask for your records to be sent to the second opinion doctor You can still ask for a second opinion even if you have already started treatment or still want to be treated by your first specialist.
Taking part in a clinical trial
Your doctor may suggest that you consider taking part in a clinical trial. Clinical trials are a vital part of the search to find better treatments for cancer. Doctors conduct clinical trials to test new or modify treatments and see if they are better than existing treatments. Many people all over the world have taken part in clinical trials that have resulted in improvements to cancer treatment. However, the decision to take part in a clinical trial is always yours.
If your doctor asks you to take part in a clinical trial, make sure that you fully understand the reasons for the trial and what it means for you. Before deciding whether or not to join the trial, you may wish to ask your doctor:
· What treatments are being tested and why?
· What tests are involved?
· What are the possible risks or side effects?
· How long will the trial last?
· Will I need to go into hospital for treatment?
· What will I do if any problems occur while I am in the trial?
If you decide to join a randomised clinical trial, you will be given the best existing treatment or a promising treatment. You will be chosen at random to receive one treatment or other, but it will always be at least the best treatment available. If you do join the clinical trial, you have the right to withdraw at any time, doing so will not jeopardise your treatment for cancer. It is always your decision to take part in a clinical trial. If you do not want to take part, your doctor will discuss the best current treatment choices with you.
Recovery and follow-up care
After the completion of your treatment, you will need to have regular checkups. Your doctor will decide how often you will need checkups, as everyone is different. They will gradually become less frequent if you have no further problems. If the disease flares up, or relapses, it can often be treated successfully. The treatment used for the relapse is often different from the first treatment.
4. Seeking Support
It is normal to feel a range of intense emotions for some time after your diagnosis and treatment. You may feel sad, depressed, angry or frustrated. It is important to acknowledge these reactions and understand that it may take some time before you feel well again. It may be helpful to talk about your feelings with your partner, family members or friends, or with a hospital counsellor, social worker, psychologist or your religious or spiritual adviser. Sometimes you may find that your friends and family do not know what to say to you: they may have difficulty with their feelings as well. Some people may feel so uncomfortable that they avoid you. They may expect you to ‘lead the way’ and tell them what you need. You may prefer to ask a close family member or a friend to talk with other people for you.
Loss of fertility can be difficult for many women to cope with, even if they already have a child or children, or have chosen not to have children. You, with or without your partner, may need to seek help to cope with your grief. This may be through a social worker, psychologist and psychiatrist or through other support services. Permanent care or adoption of a child may be a choice for some women. This requires dedication and perseverance and not all couples who wish to adopt a child are able to do so.
Diet
A balanced, nutritious diet will help you keep as well as possible and cope with the cancer and any side effects treatment. Depending on the kind of treatment you have had, you may have special dietary needs. A dietician may help plan the best foods for your particular situation; ones that you find tempting, easy to eat and nutritious. The Resource and Wellness Centre have a resident dietician. To make an appointment please call 03 2698 7300 or email contact@cancer.org.my
Exercise
You will probably find it helpful to stay active and to exercise regularly if you can. The amount and type of exercise you do will depend upon what you are used to and how well you feel.
Discuss with your doctor what is likely to be best for you.
Relaxation techniques
Some women find relaxation or meditation techniques helpful. The Resource and Wellness Centre conduct relaxation and meditation classes.
Sexuality and cancer
The diagnosis and treatment of cervical cancer may affect how you feel about yourself and your relationships. It is a time when you will need support as your relationships may change. Current or new partners may also have difficulty adjusting and may need reassurance. You may find it helpful to share your feelings with each other. However, this is not always possible as with all crises, some relationships suffer under the strain. You may both need to seek separate support.
If you need radiotherapy you are usually able to continue being sexually active during treatment, as long as it is comfortable for you and you feel like it. Everyone is different and you should be guided by how you feel. You may find that, particularly near the end of treatment, you don't feel like penetrative sex. If you have vaginal dryness, a gel such as KY Jelly can be helpful. This can be bought from a chemist or supermarket. Some women may bleed after sexual intercourse when they are having radiotherapy. Don't be worried but let your doctor or nurse know
After you have had your check-up following surgery you will be able to recommence sexual activity. However, some women find that it takes time before they feel both physically and emotionally well enough. It may be some time until you feel you are ready for sex. You may need to build up your confidence first. Sharing affection with your partner through kissing, caressing and touching can give you both much pleasure. Talking about your needs together is important to help you feel more confident and to reduce any fears.
If you are resuming vaginal intercourse, you may wish to proceed slowly. As your vagina may be a little shorter after treatment, you may find it better to try different positions for intercourse. You may want to choose a position where you have more control and there is less pressure to your pelvic area. If you have difficulty you may need expert advice.
If there are some special aids to help you gradually stretch your vagina after surgery or radiotherapy. These are called vaginal dilators and are available from your gynaecological oncologist or from specialist services like family planning clinics. If you find that you are having difficulty resuming your sexual relationship, you may need specialist help and advice. You may want to talk with your doctor about this or ask for advice on where you can get help. Remember, it is normal not to feel like sex after being treated for cancer.
Coping with side effects
It may take some time to recover from the various types of treatment. You will find that there are physical changes as well as many emotional changes to cope with. It is important that you, your partner, family and employer are prepared for this.
Premature menopause
Ovaries produce the hormones oestrogen and progesterone. If your ovaries are surgically removed or damaged by radiotherapy, they will no longer produce these hormones. This means that you will have premature menopause. Your body will have lower levels of these hormones circulating in the blood, which can cause symptoms such as hot flushes and palpitations. Oestrogen s an important protection against osteoporosis and heart disease, so premature menopause may increase your risk of these diseases.
Hormone replacement therapy (HRT) can be taken to reduce or prevent symptoms of menopause. HRT is a combination of oestrogen and progesterone, taken in tablets. You will need to discuss with your doctor, and evaluate for yourself, the benefits and possible risks of taking HRT. There are also many useful books about menopause, which may help you with your decisions.
Bladder problems
Bladder sensations or control may change after treatment. Some women find they need to go to the toilet more often; others find that they need to go in a hurry and sometimes don't get there in time. Others find that they pass urine when they cough or sneeze. While these problems may improve, even a small loss of bladder control can be upsetting. If bladder control is a problem for you, you should seek help. Your specialist will be able to suggest ways to help with bladder control. These may include special exercises to strengthen the muscles of your pelvic floor. You should also be visited in hospital by a physiotherapist who can teach you about these exercises, or you can contact The Resource and Wellness Centre.
Bowel problems
After surgery some women may have problems with their bowels for a while. This may be wind pain that can be helped by sucking strong peppermints. Other women find that they become constipated or suffer from diarrhoea and may need to make adjustments to their diet or take medication. Talk with your doctor if your bowel problems or pain do not improve.
Lymphoedema
Lymphoedema is swelling of part of the body, usually the legs or arms. It may occur after treatment for cervical cancer if you have had the lymph nodes in your pelvis removed (a lymphadenectomy). Removal of the nodes may prevent normal draining of the fluid from the legs. As a result fluid can build up in one or both legs causing swelling. This usually does not occur until some time after the original treatment.
It is not possible to predict whether you will have problems with lymphoedema. If you begin to have problems seek immediate help, as symptoms are better managed if treated early. Seek advice from your specialist or nurse. You may be given special stockings to wear after your operation.
Some hospitals have specialist physiotherapists who can advise you on how you may be able to reduce your risk of developing lymphoedema. They also help you if lymphoedema does occur in the future. For further information about lymphoedema, contact the Resource and Wellness Centre.
Cancer support groups
Cancer support groups offer mutual support and information to people with cancer and, often, to their families. It can help to talk with others who have gone through the same experience. Support groups can also offer many practical suggestions and ways of coping. For information about the Support Groups, contact the Resource and Wellness Centre.
Caring for someone with cancer
Caring for someone with cancer can be very stressful; particularly when it is someone you care about very much. Look after yourself during this time. Give yourself some time out, and share your worries and concerns with someone outside. You may have to make many decisions. You will probably have to attend many appointments with doctors, support services and hospitals. Many people have found it helpful to take with them another member of the family or a close friend. It also helps to write down questions beforehand, and to take notes during the appointment.
Cancer support group membership is generally open to patients and carers. A support group can offer the chance to share experiences and ways of coping.
Cancer Information and Support Service
The Resource and Wellness Centre is a service of the National Cancer Society of Malaysia. It is a confidential service where you can talk about your concerns and needs with specially trained staff. The staff can send you written information and can put you in touch with appropriate services in your own area. Telephone 03 2698 7300 or email contact@cancer.org.my
5. Information Checklist
1 What type of cancer do I have?
2 How extensive is my cancer?
3 What treatment do you advise for my cancer and why?
4 Will my treatment (and surgery) be performed by a doctor who specialises in cervical cancer?
5 Are there other treatment choices for me? If not, why not?
6 What are the risks and possible side effects of each treatment?
7 Will I have to stay in hospital, or will I be treated as an out patient?
8 How long will the treatment take? How much will it affect what I can do?
9 How much will it cost?
10 Will I have a lot of pain with the operation? What will be done about this?
11 If I need further treatment, what will it be like and when will it begin?
12 Will the treatment affect my sexual relationships?
13 How frequent will my check-ups be and what will they involve?
14 Are there any problems I should watch out for?
15 I would like to have a second opinion. Can you refer me to someone else?
16 Is my cancer hereditary?
If there are answers you do not understand, feel comfortable to say 'can you explain that again' or 'I am not sure what you mean by ...'
Glossary
Most of the words listed here are used on this web page, others are words you are likely to hear used by doctors and other health professionals who will be working with you.
adenocarcinoma
A cancer that has arisen in glandular cells.
anaesthetic
A drug given to stop a person feeling pain. A 'local' anaesthetic numbs part of the body; a 'general' anaesthetic cause temporary loss of consciousness.
angiogenesis
The formation of new blood vessels to support tissue. Angiogenesis enables tumours to develop their own blood supply, which helps them to survive and grow.
benign
Not cancerous. Benign cells are not able to spread like cancer cells.
biopsy
The removal of a small sample of tissue from the body, for examination under a microscope, to help diagnose a disease.
carcinoma in situ
Cancer that involves only the cells in which it began and has not spread to nearby tissues.
catheter
A flexible tube inserted into a narrow opening so that fluids can be introduced or removed.
cells
The 'building blocks' of the body. A human is made of millions of cells, which are adapted for different functions. Cells are able
to reproduce themselves exactly, unless they are a abnormal or damaged, as are cancer cells.
cervix
The lower part of the uterus, which extends into the vagina
chemotherapy
The use of special (cytotoxic) drugs to treat cancer by killing cancer cells or slowing their growth.
colposcopy
The examination of the vagina and cervix with a magnifying instrument, called a colposcope, to check these tissues for abnormality.
computerised tomography (CT) scan
The technique for constructing pictures from cross sections of the body, by x-raying the part of the body to be examined from many different angles.
cone biopsy
The removal of a cone-shaped piece of the cervix. It may be used to both diagnose and treat a problem.
dysplasia
An alteration in size, shape and arrangement of normal cells. Dysplastic cells are abnormal but are not cancerous. They may progress into cancer.
endocervical cells
The cells lining the inside of the cervix.
genes
The tiny factors that govern the way the body's cells grow and behave. Each person has a set of many thousands of genes inherited from both parents. These genes are found in every cell of the body.
gynaecological oncologist
A doctor who specialises in treating women diagnosed with cancer of the reproductive organs.
hormone replacement therapy (HRT)
Female hormones (oestrogen and progesterone) which can be taken by women to relieve symptoms of menopause.
hysterectomy
The removal of a woman's uterus by surgery.
intravenous
Into a vein. An intravenous drip gives drugs directly into a vein.
leucopoenia
A reduction in the number of white blood cells in the blood
lymphadenectomy
Removal of the lymph nodes from a particular part of the body
lymph nodes
Also called lymph glands. Small, bean-shaped structures which form part of the lymphatic system. Lymph is the fluid that flows through this system and carries cells that help to fight disease and infection. The lymph nodes filter the lymph to remove bacteria and other harmful agents, such as cancer cells.
lymph vesselS
Part of the lymphatic system. The lymphatic system is part of the immune system, which protects the body against ‘invaders’, like bacteria and parasites. The lymphatic system is a network of small lymph nodes connected by very thin lymph vessels, which branch into every part of the body.
lymphoedema
Swelling of a part of the body, usually the legs or arms. Caused by the blockage or removal of the lymph nodes so causing fluid (lymph) to accumulate.
malignant
Cancerous. Malignant cells can spread (metastasise) and can eventually cause death if they cannot be treated.
menopause
The natural cessation of a woman's periods or menstruation. This is the main event marking a woman's transition from when having children is possible to the post-reproductive years. Usually occurs between the ages of 45 and 55 years.
metastases
Also known as 'secondaries'. Tumours or masses of cells that develop when cancer cells break away from the original (primary) cancer and are carried by the lymphatic and blood systems to other parts of the body.
Pap test
A test that can detect changes in cervical cells. Some cells are scraped off the cervix and sent to a laboratory for examination under a microscope.
prognosis
An assessment of the course and likely outcome of a person's disease.
radiotherapy
The use of radiation to kill cancer cells. Radiation can be directed at a tumour from outside the body, or a radioactive source may be implanted into a tumour and the surrounding tissue.
squamous cell carcinoma
A cancer that arises in the squamous or skin-like cells of the cervix.
tumour
A new or abnormal growth of tissue on or in the body.
Ultrasound
‘Ultrasound’ is the sound waves of a very high frequency (higher than human can hear). If ultrasound is directed at the body it is reflected back differently by different types of the tissue. In an ultrasound scan, these differences are measures and used to build up pictures of structures in the body. Ultra sound pictures are usually taken by an ultrasound technician, who guides the scanning by watching the images on a screen like a television.
Note:
If you have or suspect you may have a health problem, you should consult your health care provider. We cannot advice you about the best treatment for you. You will need to discuss this with your own doctors. However, we hope this information will answer some of your questions and help you into thinking about questions you want to ask your doctors.

