
Definition
The rectum is the portion of the large bowel that lies in the pelvis, terminating at the anus. Cancer of the rectum is the disease characterized by the development of malignant cells in the lining or epithelium of the rectum. Malignant cells have changed such that they lose normal control mechanisms governing growth. These cells may invade surrounding local tissue or they may spread throughout the body and invade other organ systems.
Description
The rectum is the continuation of the colon (part of the large bowel) after it leaves the abdomen and descends into the pelvis. Anatomically, it is divided into equal thirds; the upper, mid, and lower rectum. The pelvis and other organs in the pelvis form boundaries to the rectum. Behind, or more accurately, posterior to the rectum is the sacrum (the lowest portion of the spine, closest to the pelvis).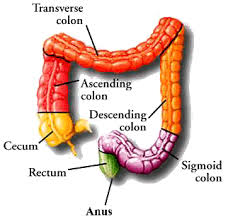
Laterally, on the sides, the rectum is bounded by soft tissue and bone. In front, the rectum is bounded by different organs in the male and female. In the male, the bladder and prostate are present. In the female, the vagina, uterus, and ovaries are present.
The upper rectum receives its blood supply from branches of the inferior mesenteric artery from the abdomen. The lower rectum has blood vessels entering from the sides of the pelvis. Lymph, a protein-rich fluid that bathes the cells of the body, is transported in small channels known as lymphatics. These channels run with the blood supply of the rectum. Lymph nodes are small filters through which the lymph flows on its way back to the blood stream. Cancer spreads elsewhere in the body by invading the lymph and vascular systems.
When a cell or cells lining the rectum become malignant, they first grow locally and may invade partially or totally through the wall of the rectum. The tumor here may invade surrounding tissue or the organs that bound it, a process known as local invasion. In this process, the tumor penetrates and may invade the lymphatics or the capillaries locally and gain access to the circulation in this way. As the malignant cells work their way to other areas of the body, they again become locally invasive in the new area to which they have spread. These tumor deposits, originating in the primary tumor in the rectum, are then known as metastasis. If metastases are found in the regional lymph nodes, they are known as regional metastases. If they are distant from the primary tumor, they are known as distant metastases. The patient with distant metastases may have widespread disease, also referred to as systemic disease. Thus the cancer originating in the rectum begins locally and, given time, may become systemic.
By the time the primary tumor is originally detected, it is usually larger than 1 cm (about 0.39 in) in size and has over a million cells. This amount of growth itself is estimated to take about three to seven years. Each time the cells double in number, the size of the tumor quadruples. Thus like most cancers, the part that is identified clinically is later in the progression than would be desired and screening becomes a very important endeavor to aid in earlier detection of this disease.
Passage of red blood with the stool, (noticeable bleeding with defecation), is much more common in rectal cancer than that originating in the colon because the tumor is much closer to the anus. Other symptoms (constipation and/ or diarrhea) are caused by obstruction and, less often, by local invasion of the tumor into pelvic organs or the sacrum. When the tumor has spread to distant sites, these metastases may cause dysfunction of the organ they have spread to. Distant metastasis usually occurs in the liver, less often to the lung(s), and rarely to the brain.
There are about 36,500 cases of rectal cancer diagnosed per year in the United States. Together, colon and rectal cancers account for 10% of cancers in men and 11% of cancers in women. It is the second most common site-specific cancer affecting both men and women. (Lung cancer is the first affecting both men and women, breast is the leader in women and prostate the leader in men.)
About 8,500 people died from rectal cancer in the United States in 2000. In recent years the incidence of this disease is decreasing very slightly, as has the mortality rate. It is difficult to tell if the decrease in mortality reflects earlier diagnosis, less death related to the actual treatment of the disease, or a combination of both factors.
Cancer of the rectum is felt to arise sporadically in about 80% of those who develop the disease. 20% of cases are felt to have genetic predisposition that ranges from familial syndromes affecting 50% of the offspring of a mutation carrier, to a risk of 6% when there is just a family history of rectal cancer occurring in a first-degree relative. Development of rectal cancer at an early age suggests a genetically transmitted form of the disease as opposed to the sporadic form.
Causes and symptoms
Causes of rectal cancer are probably environmental in the sporadic cases (80%), and genetic in the heredity-predisposed (20%) cases. Since malignant cells have a changed genetic makeup, this means that in 80% of cases, the environment spontaneously induces change. In those born with a genetic predisposition, they are either destined to get the cancer, or it will take less environmental exposure to induce the cancer. Exposure to agents in the environment that may induce mutation is the process of carcinogenesis and is caused by agents known as carcinogens. Specific carcinogens have been difficult to identify; dietary factors, however, seem to be involved.
Rectal cancer is more common in industrialized nations, and dietary factors are thought to be related to this observation. Diets high in fat, red meat, total calories, and alcohol seem to predispose. Diets high in fiber are associated with a decreased risk. The mechanism for protection by high-fiber diets may be related to less exposure of the rectal epithelium to carcinogens from the environment as the transit time through the bowel is faster with a high-fiber diet than with a low-fiber diet. Age plays a definite role in the predisposition to rectal cancer. Rectal cancer is rare before age 40. This incidence increases substantially after age 50 and doubles with each succeeding decade.
There is also a slight increase risk for rectal cancer in the individual who smokes.
Patients who suffer from an inflammatory disease of the colon known as ulcerative colitis are also at increased risk.
In regards to genetic predisposition, on chromosome 5, there is a gene called the APC gene associated with familial adenomatous polyposis (FAP) syndrome. There are multiple different mutations that occur at this site, yet they all cause a defect in tumor suppression that results in early and frequent development of colon cancer. This genetic aberration is transmitted to 50% of offspring and each of those affected will develop colon or rectal cancer, usually at an early age. Another syndrome, hereditary non-polyposis colon cancer (HNPCC), is related to mutations in any of four genes responsible for DNA mismatch repair. In patients with colon or rectal cancer, the p53 gene is mutated 70% of the time. When the p53 gene is mutated and ineffective, cells with damaged DNA escape repair or destruction, allowing the damaged cell to perpetuate itself. Continued replication of the damaged DNA may lead to tumor development. Though these syndromes (FAP and HNPCC) have a very high incidence of colon or rectal cancer, family history without the syndromes is also a substantial risk factor. When considering first-degree relatives, history of one with colon or rectal cancer raises the baseline risk of 2% to 6%, the presence of a second raises the risk to 17%.
The development of polyps of the colon or rectum commonly precedes the development of rectal cancer. Polyps are growths of the rectal lining. They can be unrelated to cancer, pre-cancerous, or malignant. Polyps, when identified, are removed for diagnosis. If the polyp, or polyps, are benign, the patient should undergo careful surveillance for the development of more polyps or the development of colon or rectal cancer.
Symptoms of rectal cancer most often result from the local presence of the tumor and its capacity to invade surrounding pelvic structure:
* bright red blood present with stool
* abdominal distention, bloating, inability to have a bowel movement
* narrowing of the stool, so-called ribbon stools
* pelvic pain
* unexplained weight loss
* persistent chronic fatigue
* rarely, urinary infection or passage of air in urine in males (late symptom)
* rarely, passage of feces through vagina in females(late symptom)
Most of the symptoms are understood on the basis of obstruction or the invasion of surrounding pelvic anatomic structures. If the tumor is large and obstructing the rectum, the patient will not be evacuating stool normally and will get bloated and have abdominal discomfort. The tumor itself may bleed and, since it is near the anus, the patient may see bright red blood on the surface of the stool. Blood alone (without stool) may also be passed. Thus, hemorrhoids are often incorrectly blamed for bleeding, delaying the diagnosis. If anemia develops, which is rare, the patient will experience chronic fatigue. If the tumor invades the bladder in the male or the vagina in the female, stool will get where it doesn't belong and cause infection or discharge. (This condition is also rare.) Patients with widespread disease lose weight secondary to the chronic illness.
If the tumor invades the bladder in the male or the vagina in the female, stool will get where it doesn't belong and cause infection or discharge. (This condition is also rare.) Patients with widespread disease lose weight secondary to the chronic illness.
Diagnosis
creening evaluation of the colon and rectum are accomplished together. Screening involves physical exam, simple laboratory tests, and the visualization of the lining of the rectum and colon. The ways to visualize the epithelium are with x rays, (indirect visualization), and endoscopy, (direct visualization).
The physical examination involves the performance of a digital rectal exam (DRE). At the time of this exam, the physician checks the stool on the examining glove with a chemical to see if any occult (invisible), blood is present. At home, after having a bowel movement, the patient is asked to swipe a sample of stool obtained with a small stick on a card. After three such specimens are on the card, the card is then easily chemically tested for occult blood also. These exams are accomplished as an easy part of a routine yearly physical exam.
Proteins are sometimes produced by cancers and these may be elevated in the patients blood. When this occurs the protein produced is known as a tumor marker. There is a tumor marker for cancer of the colon and rectum; it is known as carcinoembryonic antigen, (CEA). Unfortunately, this may be made by other adenocarcinomas as well, or it may not be produced by a particular colon or rectal cancer. Therefore, screening by chemical analysis for CEA has not been helpful. CEA has been helpful in patients treated for colon or rectal cancer if their tumor makes the protein. It is used in a follow-up role, not a screening role.
Direct visualization of the lining of the rectum is accomplished using a scope or endoscope. The physician introduces the instrument into the rectum and is able to see the epithelium of the rectum directly. A simple rigid tubular scope may be used to see the rectal epithelium; however, screening of the colon is done at the same time. The lower colon may be visualized using a fiberoptic flexible scope in a procedure known as flexible sigmoidoscopy. When the entire colon is visualized, the procedure is known as total colonoscopy. Each type of endoscopy requires pre-procedure preparation (evacuation) of the rectum and colon.
The American Cancer Society has recommended the following screening protocol for those over 50 years:
* yearly digital rectal exam with occult blood in stool testing
* flexible sigmoidoscopy at age 50
* flexible sigmoidoscopy repeated every five years
If there are predisposing factors such as positive family history, history of polyps, or a familial syndrome, screening evaluations should start sooner.
Evaluation of patients with symptoms
When patients visit their physician because they are experiencing symptoms that could possibly be related to colon or rectal cancer, the entire colon and rectum must be visualized. Even if a rectal lesion is identified, the entire colon must be screened to rule out a syndromous polyp or cancer of the colon. The combination of a flexible sigmoidoscopy and double contrast barium enema may be performed, but the much preferred evaluation of the entire colon and rectum is that of complete colonoscopy. Colonoscopy allows direct visualization, photography, as well as the opportunity to obtain a biopsy, (a sample of tissue), of any abnormality visualized. If, for technical reasons the entire colon is not visualized endoscopically, a double contrast barium enema should complement the colonoscopy. A patient who is identified to have a problem in one area of the colon or rectum is at greater risk to have a similar problem in area of the colon or rectum. Therefore the entire colon and rectum need to be visualized during the evaluation.
The diagnosis of rectal cancer is actually made by the performance of a biopsy of any abnormal lesion in the rectum. Many rectal cancers are within reach of the examiner's finger. Identifying how close to the anus the cancer has developed is very important in planning the treatment. Another characteristic ascertained by exam is whether the tumor is mobile or fixed to surrounding structure. Again, this will have implications related to primary treatment. As a general rule, it is easier to identify and adequately obtain tissue for evaluation in the rectum as opposed to the colon. This is because the lesion is closer to the anus.
If the patient presents with advanced disease, areas where the tumor has spread, such as the liver, may be amenable to biopsy. Such biopsies are usually obtained using a special needle under local anesthesia.
Once a diagnosis of rectal cancer has been established by biopsy, in addition to the physical exam, an endorectal ultrasound will be performed to assess the extent of the disease. For rectal cancer, endorectal ultrasound is the most preferred method for staging both depth of tumor penetration and local lymph node metastatic status. Endorectal ultrasound:
* differentiates areas of invasion within large rectal adenomas that seem benign
* determines the depth of tumor penetration into the rectal wall
* determines the extent of regional lymph node invasion
* can be combined with other tests (chest x rays and computed tomography scans, or CT scans) to determine the extent of cancer spread to distant organs, such as the lungs or liver
The resulting rectal cancer staging allows physicians to determine the need for-and order of-radiation, surgery, and chemotherapy.
Treatment
Once the diagnosis has been confirmed by biopsy and the endorectal ultrasound has been performed, the clinical stage of the cancer is assigned. The staging characteristics are utilized by the treating physicians to plan the specific treatment protocol for the patient. In addition, the stage of the cancer at the time of presentation gives a statistical likelihood of the treatment outcome, the prognosis.
Clinical staging
Rectal cancer first invades locally and then progresses to spread to regional lymph nodes or to other organs as noted in the description above. Using the characteristics of the primary tumor, its depth of penetration through the rectum, local invasion into pelvic structure, and the presence or absence of regional or distant metastases, stage is derived. A CT scan of the pelvis is very helpful here because the presence of invasion into the sacrum or pelvic sidewalls may mean that surgical therapy is not initially possible. On this basis, clinical staging is used to begin treatment. The pathologic stage is defined when the results of analyzing the surgical specimen are available for assigning stage, (typically stage I and II).
Rectal cancer is assigned stages I through IV, based on the following general criteria:
* Stage I: the tumor is confined to the epithelium or has not penetrated through the first layer of muscle in the rectal wall.
* Stage II: the tumor has penetrated through to the outer wall of the rectum or has gone through it, possibly invading other local tissue or organs.
* Stage III: Any depth or size of tumor associated with regional lymph node involvement.
* Stage IV: any of previous criteria associated with distant metastasis.
Surgery
The first, or primary, treatment modality utilized in the treatment of rectal cancer is surgery. Stage I, II, and even suspected stage III disease are treated by surgical removal of the involved section of the rectum along with the complete vascular and lymphatic supply. Most Stage II and Stage III rectal cancers (based on endorectal ultrasound, CT scan, and chest x ray) are treated with radiation and possibly chemotherapy prior to surgery.
A factor that needs to be considered when considering primary treatment for rectal cancer is the surgeon's ability to reconnect the ends of the rectum. The pelvis is a confining space that makes the performance of the hook-up more difficult to do safely when the tumor is in the lower rectum. The upper rectum does not usually present a substantial problem to the surgeon restoring bowel continuity after the cancer has been removed. Mid-rectal tumors, (especially in males where the pelvis is usually smaller than a woman's), may present technical difficulties in hooking the proximal bowel to the remaining rectum. Technical advances in stapling instrumentation have largely overcome these difficulties. If the anastomosis, (hook-up), leaks postoperatively, infection will ensue and in the past was a major cause of complications in resection of rectal cancers. Today, utilizing the stapling instrumentation, a hook-up at the time of original surgery is much safer. If the surgeon feels that the hook-up is compromised or may leak, a colostomy may be performed. A colostomy is performed by bringing the colon through the abdominal wall and sewing it to the skin. In these cases the stool is thus diverted away from the hook-up, allowing it to heal and preventing the infectious complications associated with leak. Later, when the hook-up has completely healed, the colostomy can be taken down and bowel continuity thus restored.
Stapling devices have allowed the surgeon to get closer to the anus and still allow the technical performance of a hook-up but there are limits. It is generally felt that there should be at least three centimeters of normal rectum below the tumor or the risk of recurrence locally will be excessive. In addition, if there is no residual native rectum, the patient will not have normal sensation or control and will have problems with uncontrollable soilage, (incontinence). For these reasons, patients presenting with low rectal tumors may undergo total removal of the rectum and anus. This procedure is known as an abdominal-perineal resection. A colostomy is performed in the lower left abdomen and it is permanent.
Radiation
As mentioned, for many late stage II or stage III tumors, radiation therapy can shrink the tumor prior to surgery. The other roles for radiation therapy are as an aid to surgical therapy in locally advanced disease that has been removed, and in the treatment of certain distant metastases. Especially when utilized in combination with chemotherapy, radiation used postoperatively has been shown to reduce the risk of local recurrence in the pelvis by 46% and death rates by 29%. Such combined therapy is recommended in patients with locally advanced primary tumors that have been removed surgically. In the treatment of distant metastases, radiation has been helpful at reducing local effects from them, particularly in the brain.
Chemotherapy
Adjuvant chemotherapy, (treating the patient who has no evidence of residual disease but who is at high risk for recurrence), is considered in patients whose tumors deeply penetrate or locally invade (late stage II and stage III). If the tumor was not locally advanced, this form of chemotherapeutic adjuvant therapy may be recommended without radiation. This therapy is identical to that of colon cancer and leads to similar results. Standard therapy is treatment with 5-fluorouracil, (5-FU) combined with leucovorin for a period of six to 12 months. 5-FU is an antimetabolite and leucovorin improves the response rate. Another agent, levamisole, (which seems to stimulate the immune system), may be substituted for leucovorin. These protocols reduce rate of recurrence by about 15% and reduce mortality by about 10%. The regimens do have some toxicity but usually are tolerated fairly well.
Similar chemotherapy is administered for stage IV disease or if a patient progresses and develops metastasis. Results show response rates of about 20%. A response is a temporary regression of the cancer in response to the chemotherapy. Unfortunately, these patients eventually succumb to the disease. Clinical trials have now shown that the results can be improved with the addition of another agent to this regimen. Irinotecan does not seem to increase toxicity but it improved response rates to 39%, added two to three months to disease free survival, and prolonged overall survival by a little over two months.
Alternative treatment
Alternative therapies have not been studied in a scientific way so it is very difficult to make any recommendation. Large doses of vitamins, fiber, and green tea are among therapies tried. Before initiating any alternative therapies, the patient is wise to consult his/her physician to be sure that these therapies do not complicate or interfere with the recommended therapy.
Prognosis
Prognosis is the long-term outlook or survival after therapy. Overall, about 50% of patients treated for colon and rectal cancer survive the disease. As expected, the survival rates are dependent upon the stage of the cancer at the time of diagnosis, making early detection a very worthwhile endeavor. About 15% of patients present with stage I disease, or are diagnosed with Stage I disease when they initially visit a doctor, and 85-90% survive. Stage II represents 20-30% of cases and 65-75% survive. 30-40% comprise the stage III presentation of which 55% survive. The remaining 20-25% present with stage IV disease and are very rarely cured.
Prevention
There is not an absolute way of preventing colon or rectal cancer. Still there is a lot that an individual can do to lessen risk or to identifiy the precursors of colon and rectal cancer so that it does not manifest itself. The patient with a familial history can enter screening and surveillance programs earlier than the general population. High-fiber diets and vitamins, avoiding obesity, and staying active lessen the risk. Avoiding cigarettes and alcohol may be helpful. By controlling these environmental factors, an individual can lessen risk and to this degree prevent the disease.
By undergoing appropriate screening when uncontrollable genetic risk factors have been identified, an individual may be rewarded by the identification of benign polyps that can be treated as opposed to having these growths degenerate into a malignancy.
Adenocarcinoma
Type of cancer beginning in glandular epithelium.
Adjuvant therapy
Treatment involving radiation, chemotherapy (drug treatment), or hormone therapy, or a combination of all three given after the primary treatment for the possibility of residual microscopic disease.
Anastomosis
Surgical re-connection of the ends of the bowel after removal of a portion of the bowel.
Anemia
The condition caused by too few circulating red blood cells, often manifest in part by fatigue.
Carcinogens
Substances in the environment that cause cancer, presumably by inducing mutations, with prolonged exposure.
Defecation
The act of having a bowel movement.
Epithelium
Cells composing the lining of an organ.
Lymphatics
Channels that are conduits for lymph.
Lymph nodes
Cellular filters through which lymphatics flow.
Malignant
Cells that have been altered such that they have lost normal control mechanisms and are capable of local invasion and spread to other areas of the body.
Metastasis
Site of invasive tumor growth that originated from a malignancy elsewhere in the body.
Mutation
A change in the genetic make up of a cell that may occur spontaneously or be environmentally induced.
Occult blood
Presence of blood that cannot be appreciated visually.
Polyps
Localized growths of the epithelium that can be benign, pre-cancerous, or harbor malignancy.
Resect
To remove surgically.
Sacrum
Posterior bony wall of the pelvis.
Systemic
Referring to throughout the body.
For Your Information
Books
* Abelhoff, Martin, MD, James O. Armitage MD, Allen S. Lichter MD, and John E. Niederhuber MD. Clinical Oncology Library. Philadelphia: Churchill Livingstone, 1999.
* Jorde, Lynn B., PhD, John C. Carey MD, Michael J. Bamshad MD, and Raymond L. White, PhD. Medical Genetics, Second Edition. St. Louis: Mosby, 1999.
* Kirkwood, John M., MD, Michael T. Lotze MD, Joyce M. Yasko PhD. Current Cancer Therapeutics, Third Edition. Philadelphia: Churchill Livingstone, 1998
Periodicals
* Greenlee, Robert T., PhD, MPH, Mary Beth Hill-Harmon, MSPH, Taylor Murray, and Michael Thun, MD, MS. "Cancer Statistics 2001." CA: A Cancer Journal for Clinicians, 51, no. 1 (Jan/Feb 2001).
* Saltz, Leonard, et al. "Irinotecan plus Fluorouracil and Leucovorin for Metastatic Colorectal Cancer." The New England Journal of Medicine 343, no. 13 (September 28, 2000).
Organizations
* American Cancer Society. 1599 Clifton Road NE, Atlanta, GA 30329. (800)ACS-2345. http://www.cancer.org.
* Cancer Information Service of the NCI. 9000 Rockville Pike, Building 31, Suite 10A18, Bethesda, MD 20892. 1-800-4-CANCER. http://wwwicic.nci.nih.gov.
Other
The Essay Author is Richard A. McCartney MD.
Source:http://www.healthatoz.com/healthatoz/Atoz/common/standard/
transform.jsp?requestURI=/healthatoz/Atoz/ency/rectal_cancer.jsp
Description
The rectum is the continuation of the colon (part of the large bowel) after it leaves the abdomen and descends into the pelvis. Anatomically, it is divided into equal thirds; the upper, mid, and lower rectum. The pelvis and other organs in the pelvis form boundaries to the rectum. Behind, or more accurately, posterior to the rectum is the sacrum (the lowest portion of the spine, closest to the pelvis).
Laterally, on the sides, the rectum is bounded by soft tissue and bone. In front, the rectum is bounded by different organs in the male and female. In the male, the bladder and prostate are present. In the female, the vagina, uterus, and ovaries are present.
The upper rectum receives its blood supply from branches of the inferior mesenteric artery from the abdomen. The lower rectum has blood vessels entering from the sides of the pelvis. Lymph, a protein-rich fluid that bathes the cells of the body, is transported in small channels known as lymphatics. These channels run with the blood supply of the rectum. Lymph nodes are small filters through which the lymph flows on its way back to the blood stream. Cancer spreads elsewhere in the body by invading the lymph and vascular systems.
When a cell or cells lining the rectum become malignant, they first grow locally and may invade partially or totally through the wall of the rectum. The tumor here may invade surrounding tissue or the organs that bound it, a process known as local invasion. In this process, the tumor penetrates and may invade the lymphatics or the capillaries locally and gain access to the circulation in this way. As the malignant cells work their way to other areas of the body, they again become locally invasive in the new area to which they have spread. These tumor deposits, originating in the primary tumor in the rectum, are then known as metastasis. If metastases are found in the regional lymph nodes, they are known as regional metastases. If they are distant from the primary tumor, they are known as distant metastases. The patient with distant metastases may have widespread disease, also referred to as systemic disease. Thus the cancer originating in the rectum begins locally and, given time, may become systemic.
By the time the primary tumor is originally detected, it is usually larger than 1 cm (about 0.39 in) in size and has over a million cells. This amount of growth itself is estimated to take about three to seven years. Each time the cells double in number, the size of the tumor quadruples. Thus like most cancers, the part that is identified clinically is later in the progression than would be desired and screening becomes a very important endeavor to aid in earlier detection of this disease.
Passage of red blood with the stool, (noticeable bleeding with defecation), is much more common in rectal cancer than that originating in the colon because the tumor is much closer to the anus. Other symptoms (constipation and/ or diarrhea) are caused by obstruction and, less often, by local invasion of the tumor into pelvic organs or the sacrum. When the tumor has spread to distant sites, these metastases may cause dysfunction of the organ they have spread to. Distant metastasis usually occurs in the liver, less often to the lung(s), and rarely to the brain.
There are about 36,500 cases of rectal cancer diagnosed per year in the United States. Together, colon and rectal cancers account for 10% of cancers in men and 11% of cancers in women. It is the second most common site-specific cancer affecting both men and women. (Lung cancer is the first affecting both men and women, breast is the leader in women and prostate the leader in men.)
About 8,500 people died from rectal cancer in the United States in 2000. In recent years the incidence of this disease is decreasing very slightly, as has the mortality rate. It is difficult to tell if the decrease in mortality reflects earlier diagnosis, less death related to the actual treatment of the disease, or a combination of both factors.
Cancer of the rectum is felt to arise sporadically in about 80% of those who develop the disease. 20% of cases are felt to have genetic predisposition that ranges from familial syndromes affecting 50% of the offspring of a mutation carrier, to a risk of 6% when there is just a family history of rectal cancer occurring in a first-degree relative. Development of rectal cancer at an early age suggests a genetically transmitted form of the disease as opposed to the sporadic form.
Causes and symptoms
Causes of rectal cancer are probably environmental in the sporadic cases (80%), and genetic in the heredity-predisposed (20%) cases. Since malignant cells have a changed genetic makeup, this means that in 80% of cases, the environment spontaneously induces change. In those born with a genetic predisposition, they are either destined to get the cancer, or it will take less environmental exposure to induce the cancer. Exposure to agents in the environment that may induce mutation is the process of carcinogenesis and is caused by agents known as carcinogens. Specific carcinogens have been difficult to identify; dietary factors, however, seem to be involved.
Rectal cancer is more common in industrialized nations, and dietary factors are thought to be related to this observation. Diets high in fat, red meat, total calories, and alcohol seem to predispose. Diets high in fiber are associated with a decreased risk. The mechanism for protection by high-fiber diets may be related to less exposure of the rectal epithelium to carcinogens from the environment as the transit time through the bowel is faster with a high-fiber diet than with a low-fiber diet. Age plays a definite role in the predisposition to rectal cancer. Rectal cancer is rare before age 40. This incidence increases substantially after age 50 and doubles with each succeeding decade.
There is also a slight increase risk for rectal cancer in the individual who smokes.
Patients who suffer from an inflammatory disease of the colon known as ulcerative colitis are also at increased risk.
In regards to genetic predisposition, on chromosome 5, there is a gene called the APC gene associated with familial adenomatous polyposis (FAP) syndrome. There are multiple different mutations that occur at this site, yet they all cause a defect in tumor suppression that results in early and frequent development of colon cancer. This genetic aberration is transmitted to 50% of offspring and each of those affected will develop colon or rectal cancer, usually at an early age. Another syndrome, hereditary non-polyposis colon cancer (HNPCC), is related to mutations in any of four genes responsible for DNA mismatch repair. In patients with colon or rectal cancer, the p53 gene is mutated 70% of the time. When the p53 gene is mutated and ineffective, cells with damaged DNA escape repair or destruction, allowing the damaged cell to perpetuate itself. Continued replication of the damaged DNA may lead to tumor development. Though these syndromes (FAP and HNPCC) have a very high incidence of colon or rectal cancer, family history without the syndromes is also a substantial risk factor. When considering first-degree relatives, history of one with colon or rectal cancer raises the baseline risk of 2% to 6%, the presence of a second raises the risk to 17%.
The development of polyps of the colon or rectum commonly precedes the development of rectal cancer. Polyps are growths of the rectal lining. They can be unrelated to cancer, pre-cancerous, or malignant. Polyps, when identified, are removed for diagnosis. If the polyp, or polyps, are benign, the patient should undergo careful surveillance for the development of more polyps or the development of colon or rectal cancer.
Symptoms of rectal cancer most often result from the local presence of the tumor and its capacity to invade surrounding pelvic structure:
* bright red blood present with stool
* abdominal distention, bloating, inability to have a bowel movement
* narrowing of the stool, so-called ribbon stools
* pelvic pain
* unexplained weight loss
* persistent chronic fatigue
* rarely, urinary infection or passage of air in urine in males (late symptom)
* rarely, passage of feces through vagina in females(late symptom)
Most of the symptoms are understood on the basis of obstruction or the invasion of surrounding pelvic anatomic structures. If the tumor is large and obstructing the rectum, the patient will not be evacuating stool normally and will get bloated and have abdominal discomfort. The tumor itself may bleed and, since it is near the anus, the patient may see bright red blood on the surface of the stool. Blood alone (without stool) may also be passed. Thus, hemorrhoids are often incorrectly blamed for bleeding, delaying the diagnosis. If anemia develops, which is rare, the patient will experience chronic fatigue.
If the tumor invades the bladder in the male or the vagina in the female, stool will get where it doesn't belong and cause infection or discharge. (This condition is also rare.) Patients with widespread disease lose weight secondary to the chronic illness.Diagnosis
creening evaluation of the colon and rectum are accomplished together. Screening involves physical exam, simple laboratory tests, and the visualization of the lining of the rectum and colon. The ways to visualize the epithelium are with x rays, (indirect visualization), and endoscopy, (direct visualization).
The physical examination involves the performance of a digital rectal exam (DRE). At the time of this exam, the physician checks the stool on the examining glove with a chemical to see if any occult (invisible), blood is present. At home, after having a bowel movement, the patient is asked to swipe a sample of stool obtained with a small stick on a card. After three such specimens are on the card, the card is then easily chemically tested for occult blood also. These exams are accomplished as an easy part of a routine yearly physical exam.
Proteins are sometimes produced by cancers and these may be elevated in the patients blood. When this occurs the protein produced is known as a tumor marker. There is a tumor marker for cancer of the colon and rectum; it is known as carcinoembryonic antigen, (CEA). Unfortunately, this may be made by other adenocarcinomas as well, or it may not be produced by a particular colon or rectal cancer. Therefore, screening by chemical analysis for CEA has not been helpful. CEA has been helpful in patients treated for colon or rectal cancer if their tumor makes the protein. It is used in a follow-up role, not a screening role.
Direct visualization of the lining of the rectum is accomplished using a scope or endoscope. The physician introduces the instrument into the rectum and is able to see the epithelium of the rectum directly. A simple rigid tubular scope may be used to see the rectal epithelium; however, screening of the colon is done at the same time. The lower colon may be visualized using a fiberoptic flexible scope in a procedure known as flexible sigmoidoscopy. When the entire colon is visualized, the procedure is known as total colonoscopy. Each type of endoscopy requires pre-procedure preparation (evacuation) of the rectum and colon.
The American Cancer Society has recommended the following screening protocol for those over 50 years:
* yearly digital rectal exam with occult blood in stool testing
* flexible sigmoidoscopy at age 50
* flexible sigmoidoscopy repeated every five years
If there are predisposing factors such as positive family history, history of polyps, or a familial syndrome, screening evaluations should start sooner.
Evaluation of patients with symptoms
When patients visit their physician because they are experiencing symptoms that could possibly be related to colon or rectal cancer, the entire colon and rectum must be visualized. Even if a rectal lesion is identified, the entire colon must be screened to rule out a syndromous polyp or cancer of the colon. The combination of a flexible sigmoidoscopy and double contrast barium enema may be performed, but the much preferred evaluation of the entire colon and rectum is that of complete colonoscopy. Colonoscopy allows direct visualization, photography, as well as the opportunity to obtain a biopsy, (a sample of tissue), of any abnormality visualized. If, for technical reasons the entire colon is not visualized endoscopically, a double contrast barium enema should complement the colonoscopy. A patient who is identified to have a problem in one area of the colon or rectum is at greater risk to have a similar problem in area of the colon or rectum. Therefore the entire colon and rectum need to be visualized during the evaluation.
The diagnosis of rectal cancer is actually made by the performance of a biopsy of any abnormal lesion in the rectum. Many rectal cancers are within reach of the examiner's finger. Identifying how close to the anus the cancer has developed is very important in planning the treatment. Another characteristic ascertained by exam is whether the tumor is mobile or fixed to surrounding structure. Again, this will have implications related to primary treatment. As a general rule, it is easier to identify and adequately obtain tissue for evaluation in the rectum as opposed to the colon. This is because the lesion is closer to the anus.
If the patient presents with advanced disease, areas where the tumor has spread, such as the liver, may be amenable to biopsy. Such biopsies are usually obtained using a special needle under local anesthesia.
Once a diagnosis of rectal cancer has been established by biopsy, in addition to the physical exam, an endorectal ultrasound will be performed to assess the extent of the disease. For rectal cancer, endorectal ultrasound is the most preferred method for staging both depth of tumor penetration and local lymph node metastatic status. Endorectal ultrasound:
* differentiates areas of invasion within large rectal adenomas that seem benign
* determines the depth of tumor penetration into the rectal wall
* determines the extent of regional lymph node invasion
* can be combined with other tests (chest x rays and computed tomography scans, or CT scans) to determine the extent of cancer spread to distant organs, such as the lungs or liver
The resulting rectal cancer staging allows physicians to determine the need for-and order of-radiation, surgery, and chemotherapy.
Treatment
Once the diagnosis has been confirmed by biopsy and the endorectal ultrasound has been performed, the clinical stage of the cancer is assigned. The staging characteristics are utilized by the treating physicians to plan the specific treatment protocol for the patient. In addition, the stage of the cancer at the time of presentation gives a statistical likelihood of the treatment outcome, the prognosis.
Clinical staging
Rectal cancer first invades locally and then progresses to spread to regional lymph nodes or to other organs as noted in the description above. Using the characteristics of the primary tumor, its depth of penetration through the rectum, local invasion into pelvic structure, and the presence or absence of regional or distant metastases, stage is derived. A CT scan of the pelvis is very helpful here because the presence of invasion into the sacrum or pelvic sidewalls may mean that surgical therapy is not initially possible. On this basis, clinical staging is used to begin treatment. The pathologic stage is defined when the results of analyzing the surgical specimen are available for assigning stage, (typically stage I and II).
Rectal cancer is assigned stages I through IV, based on the following general criteria:
* Stage I: the tumor is confined to the epithelium or has not penetrated through the first layer of muscle in the rectal wall.
* Stage II: the tumor has penetrated through to the outer wall of the rectum or has gone through it, possibly invading other local tissue or organs.
* Stage III: Any depth or size of tumor associated with regional lymph node involvement.
* Stage IV: any of previous criteria associated with distant metastasis.
Surgery
The first, or primary, treatment modality utilized in the treatment of rectal cancer is surgery. Stage I, II, and even suspected stage III disease are treated by surgical removal of the involved section of the rectum along with the complete vascular and lymphatic supply. Most Stage II and Stage III rectal cancers (based on endorectal ultrasound, CT scan, and chest x ray) are treated with radiation and possibly chemotherapy prior to surgery.
A factor that needs to be considered when considering primary treatment for rectal cancer is the surgeon's ability to reconnect the ends of the rectum. The pelvis is a confining space that makes the performance of the hook-up more difficult to do safely when the tumor is in the lower rectum. The upper rectum does not usually present a substantial problem to the surgeon restoring bowel continuity after the cancer has been removed. Mid-rectal tumors, (especially in males where the pelvis is usually smaller than a woman's), may present technical difficulties in hooking the proximal bowel to the remaining rectum. Technical advances in stapling instrumentation have largely overcome these difficulties. If the anastomosis, (hook-up), leaks postoperatively, infection will ensue and in the past was a major cause of complications in resection of rectal cancers. Today, utilizing the stapling instrumentation, a hook-up at the time of original surgery is much safer. If the surgeon feels that the hook-up is compromised or may leak, a colostomy may be performed. A colostomy is performed by bringing the colon through the abdominal wall and sewing it to the skin. In these cases the stool is thus diverted away from the hook-up, allowing it to heal and preventing the infectious complications associated with leak. Later, when the hook-up has completely healed, the colostomy can be taken down and bowel continuity thus restored.
Stapling devices have allowed the surgeon to get closer to the anus and still allow the technical performance of a hook-up but there are limits. It is generally felt that there should be at least three centimeters of normal rectum below the tumor or the risk of recurrence locally will be excessive. In addition, if there is no residual native rectum, the patient will not have normal sensation or control and will have problems with uncontrollable soilage, (incontinence). For these reasons, patients presenting with low rectal tumors may undergo total removal of the rectum and anus. This procedure is known as an abdominal-perineal resection. A colostomy is performed in the lower left abdomen and it is permanent.
Radiation
As mentioned, for many late stage II or stage III tumors, radiation therapy can shrink the tumor prior to surgery. The other roles for radiation therapy are as an aid to surgical therapy in locally advanced disease that has been removed, and in the treatment of certain distant metastases. Especially when utilized in combination with chemotherapy, radiation used postoperatively has been shown to reduce the risk of local recurrence in the pelvis by 46% and death rates by 29%. Such combined therapy is recommended in patients with locally advanced primary tumors that have been removed surgically. In the treatment of distant metastases, radiation has been helpful at reducing local effects from them, particularly in the brain.
Chemotherapy
Adjuvant chemotherapy, (treating the patient who has no evidence of residual disease but who is at high risk for recurrence), is considered in patients whose tumors deeply penetrate or locally invade (late stage II and stage III). If the tumor was not locally advanced, this form of chemotherapeutic adjuvant therapy may be recommended without radiation. This therapy is identical to that of colon cancer and leads to similar results. Standard therapy is treatment with 5-fluorouracil, (5-FU) combined with leucovorin for a period of six to 12 months. 5-FU is an antimetabolite and leucovorin improves the response rate. Another agent, levamisole, (which seems to stimulate the immune system), may be substituted for leucovorin. These protocols reduce rate of recurrence by about 15% and reduce mortality by about 10%. The regimens do have some toxicity but usually are tolerated fairly well.
Similar chemotherapy is administered for stage IV disease or if a patient progresses and develops metastasis. Results show response rates of about 20%. A response is a temporary regression of the cancer in response to the chemotherapy. Unfortunately, these patients eventually succumb to the disease. Clinical trials have now shown that the results can be improved with the addition of another agent to this regimen. Irinotecan does not seem to increase toxicity but it improved response rates to 39%, added two to three months to disease free survival, and prolonged overall survival by a little over two months.
Alternative treatment
Alternative therapies have not been studied in a scientific way so it is very difficult to make any recommendation. Large doses of vitamins, fiber, and green tea are among therapies tried. Before initiating any alternative therapies, the patient is wise to consult his/her physician to be sure that these therapies do not complicate or interfere with the recommended therapy.
Prognosis
Prognosis is the long-term outlook or survival after therapy. Overall, about 50% of patients treated for colon and rectal cancer survive the disease. As expected, the survival rates are dependent upon the stage of the cancer at the time of diagnosis, making early detection a very worthwhile endeavor. About 15% of patients present with stage I disease, or are diagnosed with Stage I disease when they initially visit a doctor, and 85-90% survive. Stage II represents 20-30% of cases and 65-75% survive. 30-40% comprise the stage III presentation of which 55% survive. The remaining 20-25% present with stage IV disease and are very rarely cured.
Prevention
There is not an absolute way of preventing colon or rectal cancer. Still there is a lot that an individual can do to lessen risk or to identifiy the precursors of colon and rectal cancer so that it does not manifest itself. The patient with a familial history can enter screening and surveillance programs earlier than the general population. High-fiber diets and vitamins, avoiding obesity, and staying active lessen the risk. Avoiding cigarettes and alcohol may be helpful. By controlling these environmental factors, an individual can lessen risk and to this degree prevent the disease.
By undergoing appropriate screening when uncontrollable genetic risk factors have been identified, an individual may be rewarded by the identification of benign polyps that can be treated as opposed to having these growths degenerate into a malignancy.
Adenocarcinoma
Type of cancer beginning in glandular epithelium.
Adjuvant therapy
Treatment involving radiation, chemotherapy (drug treatment), or hormone therapy, or a combination of all three given after the primary treatment for the possibility of residual microscopic disease.
Anastomosis
Surgical re-connection of the ends of the bowel after removal of a portion of the bowel.
Anemia
The condition caused by too few circulating red blood cells, often manifest in part by fatigue.
Carcinogens
Substances in the environment that cause cancer, presumably by inducing mutations, with prolonged exposure.
Defecation
The act of having a bowel movement.
Epithelium
Cells composing the lining of an organ.
Lymphatics
Channels that are conduits for lymph.
Lymph nodes
Cellular filters through which lymphatics flow.
Malignant
Cells that have been altered such that they have lost normal control mechanisms and are capable of local invasion and spread to other areas of the body.
Metastasis
Site of invasive tumor growth that originated from a malignancy elsewhere in the body.
Mutation
A change in the genetic make up of a cell that may occur spontaneously or be environmentally induced.
Occult blood
Presence of blood that cannot be appreciated visually.
Polyps
Localized growths of the epithelium that can be benign, pre-cancerous, or harbor malignancy.
Resect
To remove surgically.
Sacrum
Posterior bony wall of the pelvis.
Systemic
Referring to throughout the body.
For Your Information
Books
* Abelhoff, Martin, MD, James O. Armitage MD, Allen S. Lichter MD, and John E. Niederhuber MD. Clinical Oncology Library. Philadelphia: Churchill Livingstone, 1999.
* Jorde, Lynn B., PhD, John C. Carey MD, Michael J. Bamshad MD, and Raymond L. White, PhD. Medical Genetics, Second Edition. St. Louis: Mosby, 1999.
* Kirkwood, John M., MD, Michael T. Lotze MD, Joyce M. Yasko PhD. Current Cancer Therapeutics, Third Edition. Philadelphia: Churchill Livingstone, 1998
Periodicals
* Greenlee, Robert T., PhD, MPH, Mary Beth Hill-Harmon, MSPH, Taylor Murray, and Michael Thun, MD, MS. "Cancer Statistics 2001." CA: A Cancer Journal for Clinicians, 51, no. 1 (Jan/Feb 2001).
* Saltz, Leonard, et al. "Irinotecan plus Fluorouracil and Leucovorin for Metastatic Colorectal Cancer." The New England Journal of Medicine 343, no. 13 (September 28, 2000).
Organizations
* American Cancer Society. 1599 Clifton Road NE, Atlanta, GA 30329. (800)ACS-2345. http://www.cancer.org.
* Cancer Information Service of the NCI. 9000 Rockville Pike, Building 31, Suite 10A18, Bethesda, MD 20892. 1-800-4-CANCER. http://wwwicic.nci.nih.gov.
Other
* National Cancer Institute Clinical Trials. http://www.cancertrials.nci.nih.gov.
* Colon Cancer Alliance. http://www.ccalliance.org.
* Colon Cancer Alliance. http://www.ccalliance.org.
The Essay Author is Richard A. McCartney MD.
Source:http://www.healthatoz.com/healthatoz/Atoz/common/standard/
transform.jsp?requestURI=/healthatoz/Atoz/ency/rectal_cancer.jsp

